

Comparative outcome analysis of home-initiated non-medical interventions among toddlers with orally ingested substances
- PMID: 26373531
- PMCID: PMC4570254
- DOI: 10.1186/s13052-015-0170-2
Comparative outcome analysis of home-initiated non-medical interventions among toddlers with orally ingested substances
Abstract
Background: Poison management guidelines recommend contacting or visiting poison centers directly after exposure. However, some parents initiated non-medical interventions on their children before visiting these centers. Aim was to evaluate the clinical and hospital outcomes of such practices among toddlers with orally ingested medication or chemical substances at a tertiary care facility.
Methods: Retrospective cohort, based on four-arm outcome analysis. Exposures were gender, age, body mass index, arrival time to facility (hours) presented in Median [Interquartile range]. Clinical outcomes were vital signs, physical examination, diagnostic tests; Hospital outcomes were in-hospital admission, length of hospital stay (hours) presented in Median [Interquartile range], hospital cost ($US). Bivariate analysis (nonparametric tests), binary logistic/linear regression were conducted. Significance at p < 0.05.
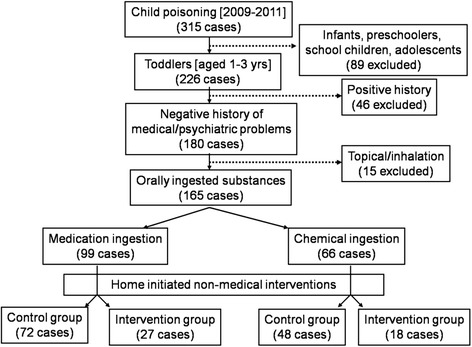
Results: Between 2009-2011, 165 (all previously healthy) toddlers were (Males = 58 %, females = 42 %) and had normal weights in 70 %. Witnessed incidents were in 85 %. Two control groups [Medication (control) = 72, Chemical (control) = 48] directly visited the facility after incident, while two intervention groups [Medication (intervention) = 27, Chemical (intervention) = 18] received orally administered water, salt/sugar solutes, milk/yogurt, lemon juice and/or manually induced vomiting before the visit. Abnormal clinical outcomes in total were in vital signs = 15 %, physical examination = 42 % and diagnostic tests = 26 %; hospital outcomes were admission = 16 %, length of stay range (2 hours-7.5 days), cost range (667-11,500). Bivariate analysis: Length of stay in Medication (intervention) = 9[5.4-12.0] hours significantly higher than Medication (control) = 5[2.7-7.5] hours, p = 0.003; abnormal physical examination in Chemical (intervention) = 77.8 % significantly higher than Chemical (control) = 37.5 %, p = 0.004. In regression: intervention significantly increased length of stay (t = 0.213, adj. P = 0.035); lower weight toddlers were at higher risk of admission (Beta = -0.51, adj. P = 0.018); delayed arrival time significantly increased abnormal physical examination (Beta = 0.29, adj. P = 0.003). No significant control/intervention group differences regarding abnormal vital signs (adj. P = 0.148), physical examination (adj. P = 0.781), diagnostic tests (adj. P = 0.285), admission (adj. P = 0.499), and cost (adj. P = 0.102).
Conclusion: Home-initiated non-medical interventions didn't improve the clinical and hospital outcomes. It has delayed the arrival time to emergency department, which added the risk of encountering abnormal physical examination, and in return increased the average length of hospital stay.
Figures
References
-
- Litovitz T, White NC, Watson WA. Epidemiology of pediatric poison exposures: an analysis of 2003 poison control center data. Clin Pediatr Emerg Med. 2005;6(2):68–75. doi: 10.1016/j.cpem.2005.04.001. - DOI
-
- McGregor T, Parkar M, Rao S. Evaluation and management of common childhood poisonings. Am Fam Physician. 2009;79(5):397–403. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
