

PD-L1 and HLA Class I Antigen Expression and Clinical Course of the Disease in Intrahepatic Cholangiocarcinoma
- PMID: 26373575
- PMCID: PMC5296951
- DOI: 10.1158/1078-0432.CCR-15-0715
PD-L1 and HLA Class I Antigen Expression and Clinical Course of the Disease in Intrahepatic Cholangiocarcinoma
Abstract
Purpose: More effective therapy is needed for intrahepatic cholangiocarcinoma (ICC). The encouraging clinical results obtained with checkpoint molecule-specific monoclonal antibodies (mAb) have prompted us to investigate whether this type of immunotherapy may be applicable to ICC. The aims of this study were to determine whether (i) patients mount a T-cell immune response to their ICC, (ii) checkpoint molecules are expressed on both T cells and tumor cells, and (iii) tumor cells are susceptible to recognition by cognate T cells.
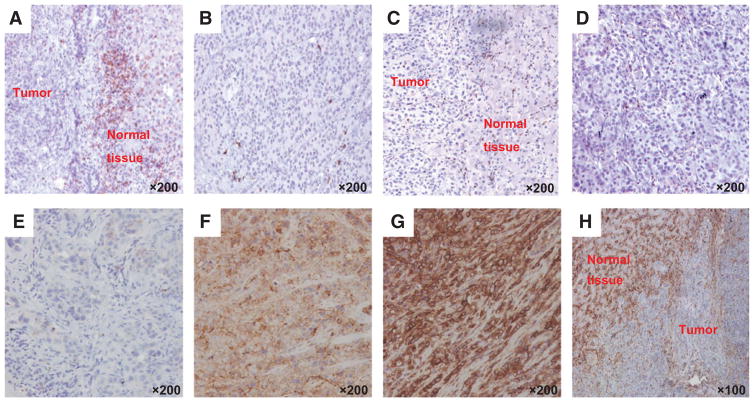
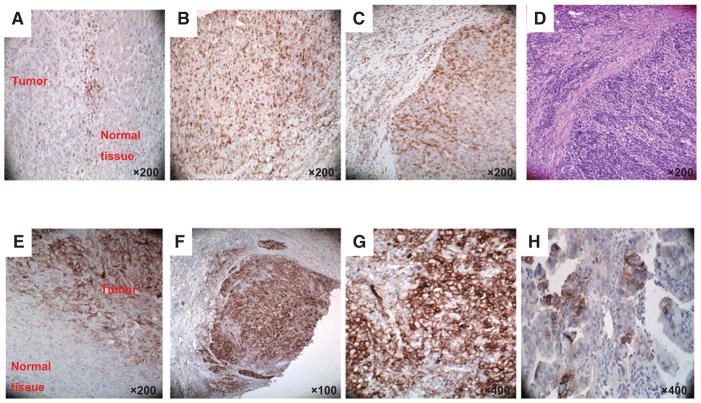
Experimental design: Twenty-seven ICC tumors were analyzed for (i) lymphocyte infiltrate, (ii) HLA class I and HLA class II expression, and (iii) PD-1 and PD-L1 expression by T cells and ICC cells, respectively. The results of this analysis were correlated with the clinicopathologic characteristics of the patients investigated.
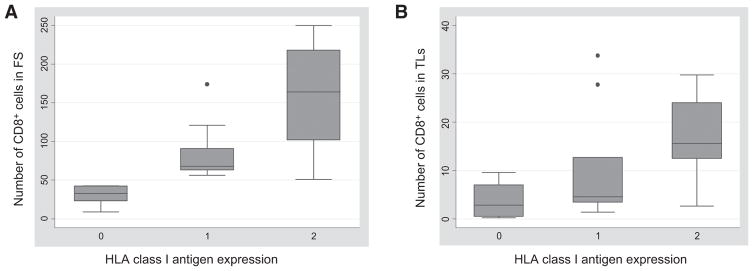
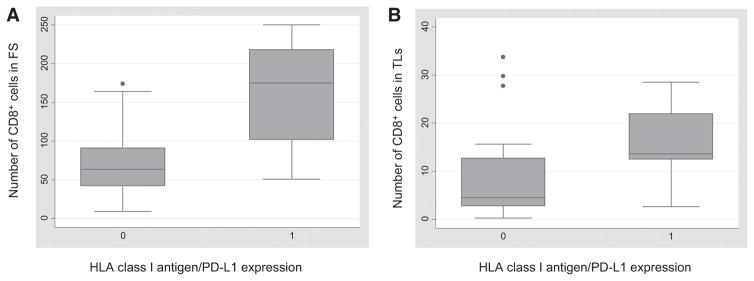
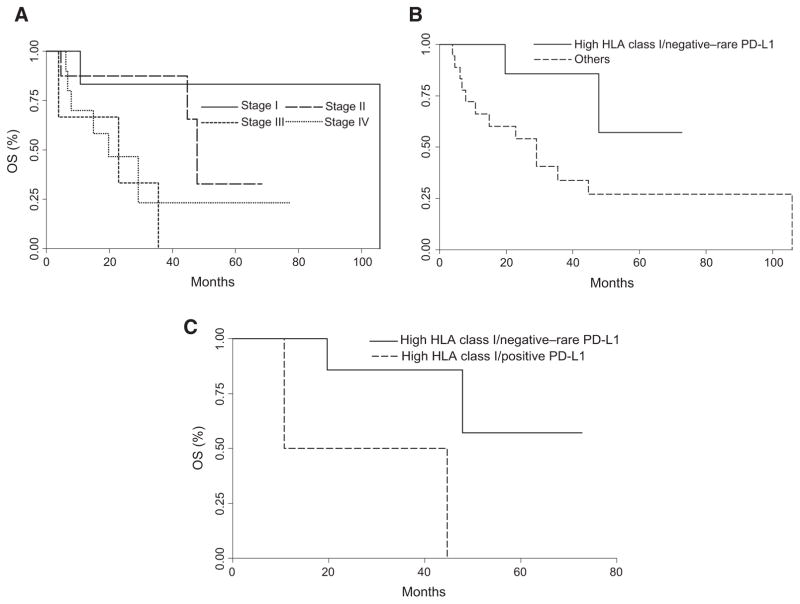
Results: Lymphocyte infiltrates were identified in all tumors. PD-L1 expression and HLA class I antigen expression by ICC cells was observed in 8 and 11, respectively, of the 27 tumors analyzed. HLA class I antigen expression correlated with CD8(+) T-cell infiltrate. Furthermore, positive HLA class I antigen expression in combination with negative/rare PD-L1 expression was associated with favorable clinical course of the disease.
Conclusions: ICC patients are likely to mount a T-cell immune response against their own tumors. Defects in HLA class I antigen expression in combination with PD-L1 expression by ICC cells provide them with an immune escape mechanism. This mechanism justifies the implementation of immunotherapy with checkpoint molecule-specific mAbs in patients bearing ICC tumors without defects in HLA class I antigen expression.
©2015 American Association for Cancer Research.
Conflict of interest statement
of Potential Conflicts of Interest No potential conflicts of interest were disclosed.
Figures
Similar articles
-
Clinical prognosticators and targets in the immune microenvironment of intrahepatic cholangiocarcinoma.Oncoimmunology. 2024 Oct 1;13(1):2406052. doi: 10.1080/2162402X.2024.2406052. eCollection 2024. Oncoimmunology. 2024. PMID: 39359389 Free PMC article.
-
HHLA2 in intrahepatic cholangiocarcinoma: an immune checkpoint with prognostic significance and wider expression compared with PD-L1.J Immunother Cancer. 2019 Mar 18;7(1):77. doi: 10.1186/s40425-019-0554-8. J Immunother Cancer. 2019. PMID: 30885276 Free PMC article.
-
Prognostic impact of CD8+ T cell distribution and its association with the HLA class I expression in intrahepatic cholangiocarcinoma.Surg Today. 2020 Aug;50(8):931-940. doi: 10.1007/s00595-020-01967-y. Epub 2020 Feb 10. Surg Today. 2020. PMID: 32040618
-
Immunotherapy for the treatment of breast cancer: checkpoint blockade, cancer vaccines, and future directions in combination immunotherapy.Clin Adv Hematol Oncol. 2016 Nov;14(11):922-933. Clin Adv Hematol Oncol. 2016. PMID: 27930644 Review.
-
TEIPP antigens for T-cell based immunotherapy of immune-edited HLA class Ilow cancers.Mol Immunol. 2019 Sep;113:43-49. doi: 10.1016/j.molimm.2018.03.029. Epub 2018 Apr 4. Mol Immunol. 2019. PMID: 29627136 Review.
Cited by
-
Novel Pharmacological Options in the Treatment of Cholangiocarcinoma: Mechanisms of Resistance.Cancers (Basel). 2021 May 13;13(10):2358. doi: 10.3390/cancers13102358. Cancers (Basel). 2021. PMID: 34068398 Free PMC article. Review.
-
MicroRNAs as Immunotherapy Targets for Treating Gastroenterological Cancers.Can J Gastroenterol Hepatol. 2018 Jun 26;2018:9740357. doi: 10.1155/2018/9740357. eCollection 2018. Can J Gastroenterol Hepatol. 2018. PMID: 30046565 Free PMC article. Review.
-
The tumour microenvironment and immune milieu of cholangiocarcinoma.Liver Int. 2019 May;39 Suppl 1(Suppl 1):63-78. doi: 10.1111/liv.14098. Liver Int. 2019. PMID: 30907492 Free PMC article. Review.
-
PD-L1 expression and presence of TILs in small intestinal neuroendocrine tumours.Oncotarget. 2018 Feb 12;9(19):14922-14938. doi: 10.18632/oncotarget.24464. eCollection 2018 Mar 13. Oncotarget. 2018. PMID: 29599916 Free PMC article.
-
Identification of neoantigen-reactive T lymphocytes in the peripheral blood of a patient with glioblastoma.J Immunother Cancer. 2021 Jul;9(7):e002882. doi: 10.1136/jitc-2021-002882. J Immunother Cancer. 2021. PMID: 34266885 Free PMC article.
References
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–25. - PubMed
-
- Yachimski P, Pratt DS. Cholangiocarcinoma: natural history, treatment, and strategies for surveillance in high-risk patients. J Clin Gastroenterol. 2008;42:178–90. - PubMed
-
- Endo I, Gonen M, Yopp AC, Dalal KM, Zhou Q, Klimstra D, et al. Intrahepatic cholangiocarcinoma: rising frequency, improved survival, and determinants of outcome after resection. Ann Surg. 2008;248:84–96. - PubMed
-
- Chouaib S. At the crossroads of cancer. Bull Cancer. 2013;100:569–74. - PubMed
-
- Armand P, Nagler A, Weller EA, Devine SM, Avigan DE, Chen YB, et al. Disabling immune tolerance by programmed death-1 blockade with pidilizumab after autologous hematopoietic stem cell transplantation for diffuse large B-cell lymphoma: Results of an international phase II trial. J Clin Oncol. 2013;31:4199–206. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
