

Inferior vena cava anomalies and variations: imaging and rare clinical findings
- PMID: 26373648
- PMCID: PMC4656244
- DOI: 10.1007/s13244-015-0431-z
Inferior vena cava anomalies and variations: imaging and rare clinical findings
Abstract
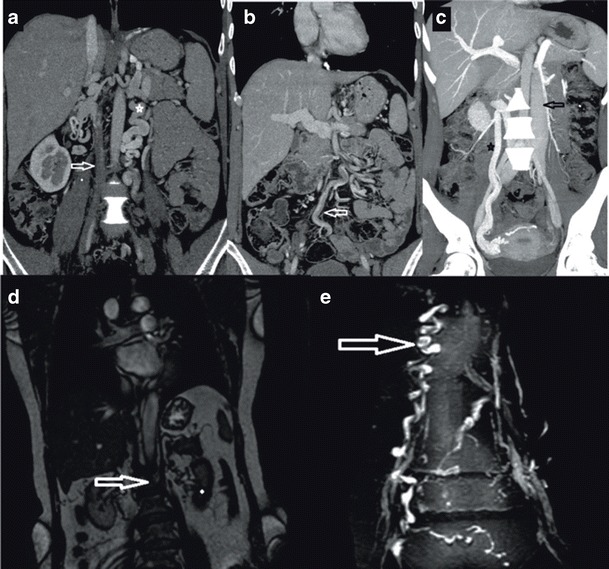
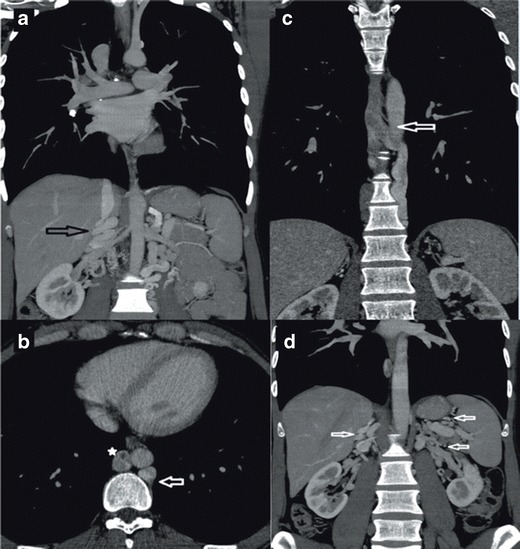
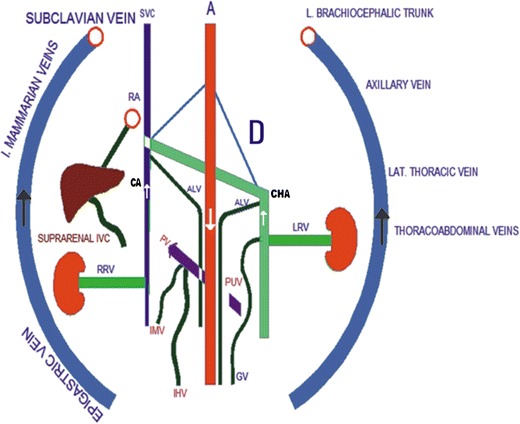
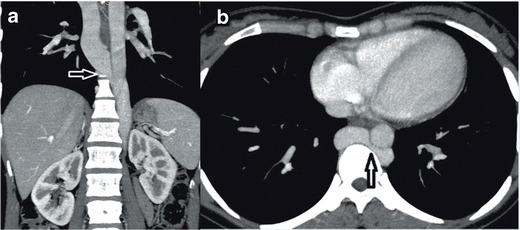
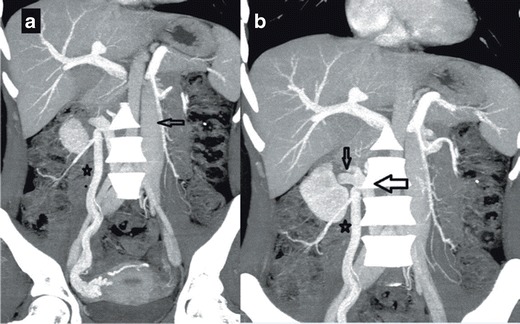
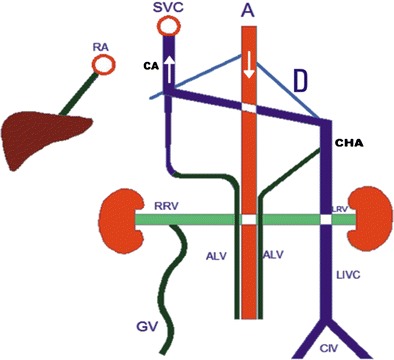
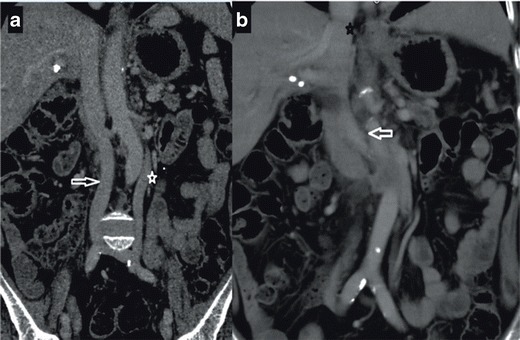
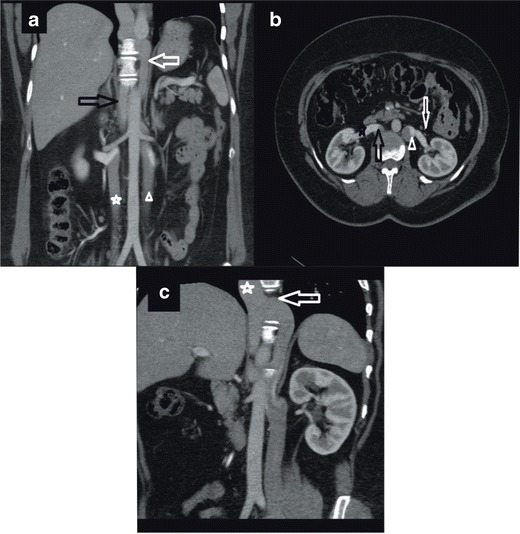
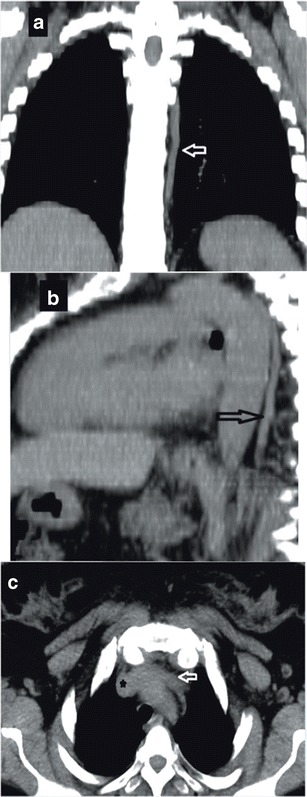
Purpose: The aim of this paper is to summarize imaging findings of some frequent and infrequent inferior vena cava (IVC) anomalies and variations.
Conclusions: IVC anomalies should be suspected in patients presenting with pulmonary emboli, chronic pain, and deep vein thrombosis. To correctly characterize and classify IVC anomalies and variations is of crucial importance for proper planning of surgical interventions and thus for avoiding serious complications.
Key points: • IVC anomalies should be suspected in patients with pulmonary emboli, pain, and venous thrombosis. • Awareness of IVC anomalies and variations is crucial for clinical and surgical procedures. • Unawareness of these anomalies may lead to severe and deadly complications.
Keywords: IVC; Inferior vena cava anomalies; Inferior vena cava variations; Magnetic resonance imaging; Multidetector row computed tomography.
Figures

References
-
- Abernethy J, Banks J. Account of two instances of uncommon formation, in the viscera of the human body. By Mr. John Abernethy, Assistant Surgeon to St. Bartholomew’s Hospital. Communicated by Sir Joseph Banks, Bart. PRS Phil Trans R Soc Lond. 1793;83:59–66. doi: 10.1098/rstl.1793.0010. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
