

Comparison of techniques for volumetric analysis of the future liver remnant: implications for major hepatic resections
- PMID: 26373675
- PMCID: PMC4644356
- DOI: 10.1111/hpb.12480
Comparison of techniques for volumetric analysis of the future liver remnant: implications for major hepatic resections
Abstract
Objective: The purpose of this work was to compare measured and estimated volumetry prior to liver resection.
Methods: Data for consecutive patients submitted to major liver resection for colorectal liver metastases at two centres during 2004-2012 were reviewed. All patients underwent volumetric analysis to define the measured total liver volume (mTLV) and measured future liver remnant ratio (mR(FLR)). The estimated total liver volume (eTLV) standardized to body surface area and estimated future liver remnant ratio (eR(FLR)) were calculated. Descriptive statistics were generated and compared. A difference between mR(FLR) and eR(FLR) of ±5% was considered clinically relevant.
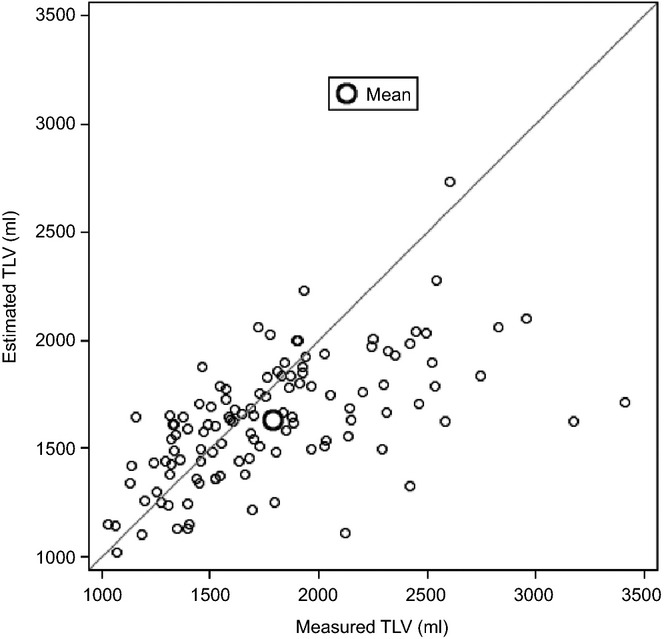
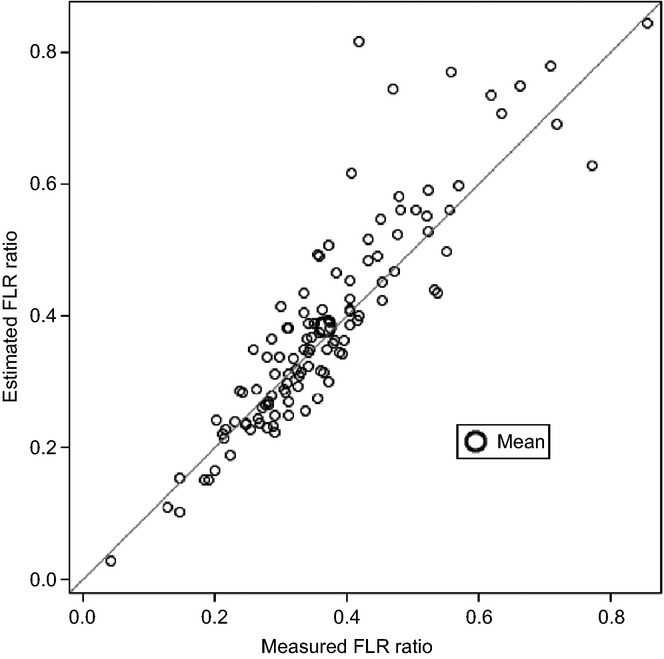
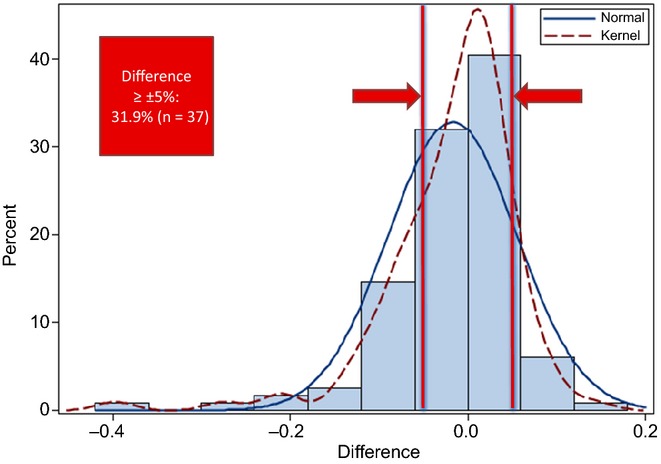
Results: Data for a total of 116 patients were included. All patients underwent major resection and 51% underwent portal vein embolization. The mean difference between mTLV and eTLV was 157 ml (P < 0.0001), whereas the mean difference between mR(FLR) and eR(FLR) was -1.7% (P = 0.013). By linear regression, eTLV was only moderately predictive of mTLV (R(2) = 0.35). The distribution of differences between mR(FLR) and eR(FLR) demonstrated that the formula over- or underestimated mR(FLR) by ≥5% in 31.9% of patients.
Conclusions: Measured and estimated volumetry yielded differences in the FLR of ≥5% in almost one-third of patients, potentially affecting clinical decision making. Estimated volumetry should be used cautiously and cannot be recommended for general use.
© 2015 International Hepato-Pancreato-Biliary Association.
Figures
Comment in
-
Re "Comparison of techniques for volumetric analysis of the future liver remnant: implications for major hepatic resections".HPB (Oxford). 2016 Jun;18(6):557. doi: 10.1016/j.hpb.2016.02.008. Epub 2016 Mar 22. HPB (Oxford). 2016. PMID: 27317961 Free PMC article. No abstract available.
References
-
- Clavien PA, Oberkofler CE, Raptis DA, Lehman K, Rickenbacher A, El-Badry AM. What is critical for liver surgery and partial liver transplantation: size or quality? Hepatology. 2010;52:715–729. - PubMed
-
- Hammond JS, Guha IN, Beckingham IJ, Lobo DN. Prediction, prevention and management of postresection liver failure. Br J Surg. 2011;98:1188–1200. - PubMed
-
- Dahm F, Georgiev P, Clavien PA. Small-for-size syndrome after partial liver transplantation: definitions, mechanisms of disease and clinical implications. Am J Transplant. 2005;5:2605–2610. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
