

Discordant identification of pediatric severe sepsis by research and clinical definitions in the SPROUT international point prevalence study
- PMID: 26373923
- PMCID: PMC4572676
- DOI: 10.1186/s13054-015-1055-x
Discordant identification of pediatric severe sepsis by research and clinical definitions in the SPROUT international point prevalence study
Abstract
Introduction: Consensus criteria for pediatric severe sepsis have standardized enrollment for research studies. However, the extent to which critically ill children identified by consensus criteria reflect physician diagnosis of severe sepsis, which underlies external validity for pediatric sepsis research, is not known. We sought to determine the agreement between physician diagnosis and consensus criteria to identify pediatric patients with severe sepsis across a network of international pediatric intensive care units (PICUs).
Methods: We conducted a point prevalence study involving 128 PICUs in 26 countries across 6 continents. Over the course of 5 study days, 6925 PICU patients <18 years of age were screened, and 706 with severe sepsis defined either by physician diagnosis or on the basis of 2005 International Pediatric Sepsis Consensus Conference consensus criteria were enrolled. The primary endpoint was agreement of pediatric severe sepsis between physician diagnosis and consensus criteria as measured using Cohen's κ. Secondary endpoints included characteristics and clinical outcomes for patients identified using physician diagnosis versus consensus criteria.
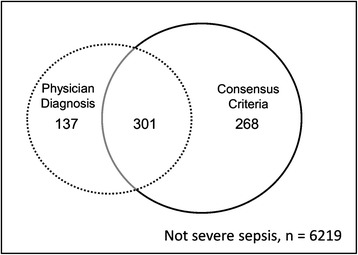
Results: Of the 706 patients, 301 (42.6%) met both definitions. The inter-rater agreement (κ ± SE) between physician diagnosis and consensus criteria was 0.57 ± 0.02. Of the 438 patients with a physician's diagnosis of severe sepsis, only 69% (301 of 438) would have been eligible to participate in a clinical trial of pediatric severe sepsis that enrolled patients based on consensus criteria. Patients with physician-diagnosed severe sepsis who did not meet consensus criteria were younger and had lower severity of illness and lower PICU mortality than those meeting consensus criteria or both definitions. After controlling for age, severity of illness, number of comorbid conditions, and treatment in developed versus resource-limited regions, patients identified with severe sepsis by physician diagnosis alone or by consensus criteria alone did not have PICU mortality significantly different from that of patients identified by both physician diagnosis and consensus criteria.
Conclusions: Physician diagnosis of pediatric severe sepsis achieved only moderate agreement with consensus criteria, with physicians diagnosing severe sepsis more broadly. Consequently, the results of a research study based on consensus criteria may have limited generalizability to nearly one-third of PICU patients diagnosed with severe sepsis.
Figures
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med. 2013;14:868–693. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
