

Intravenous Followed by X-ray Fused with MRI-Guided Transendocardial Mesenchymal Stem Cell Injection Improves Contractility Reserve in a Swine Model of Myocardial Infarction
- PMID: 26374144
- PMCID: PMC5006679
- DOI: 10.1007/s12265-015-9654-0
Intravenous Followed by X-ray Fused with MRI-Guided Transendocardial Mesenchymal Stem Cell Injection Improves Contractility Reserve in a Swine Model of Myocardial Infarction
Abstract
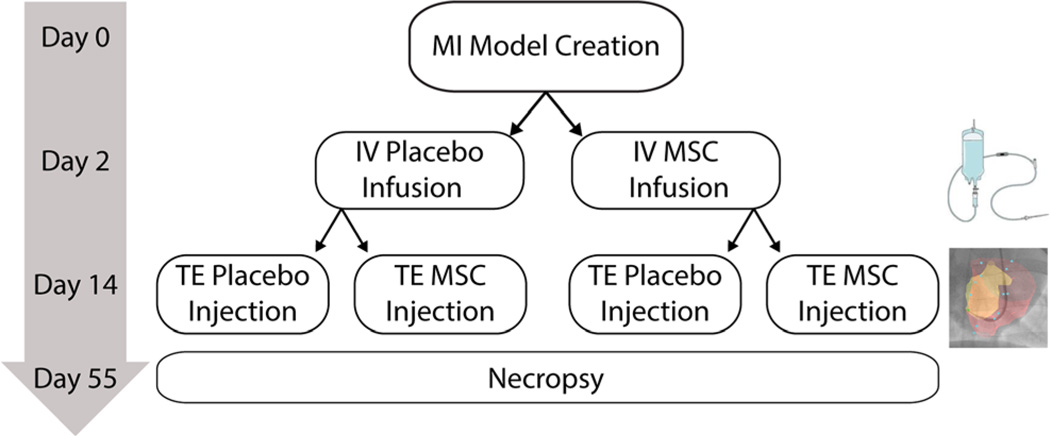
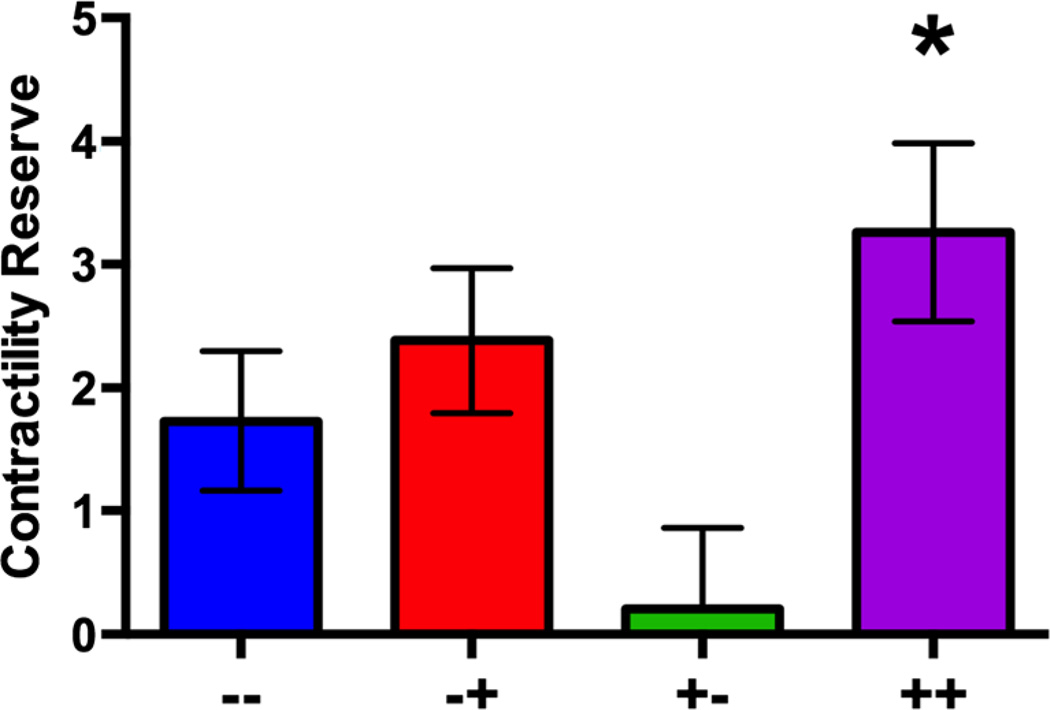
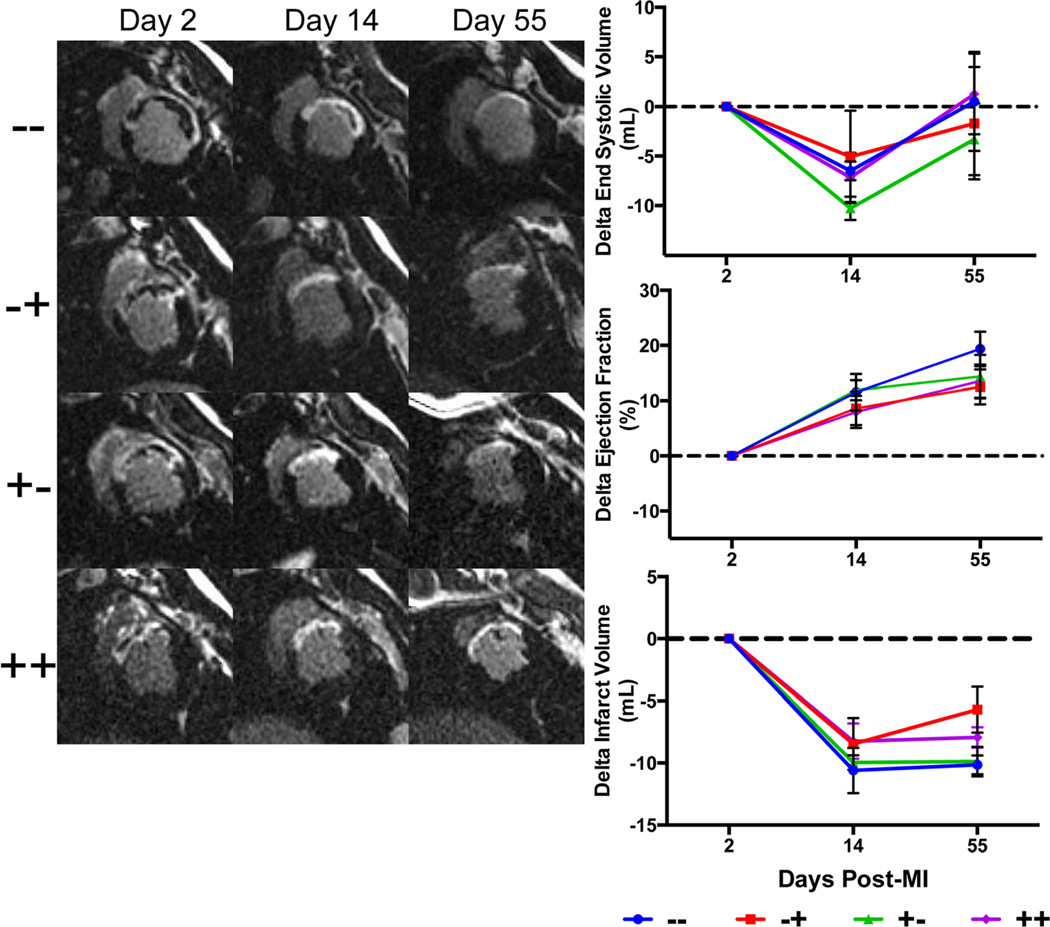
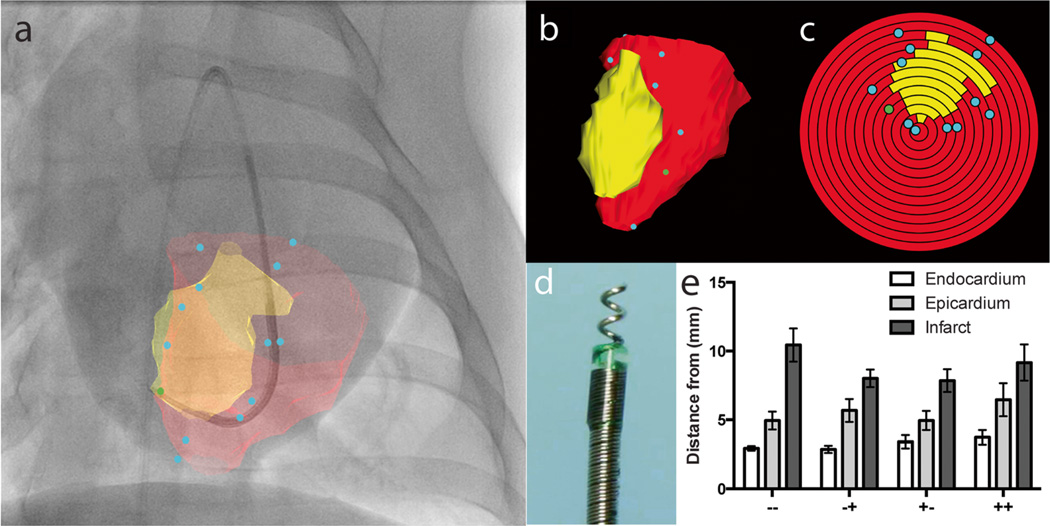
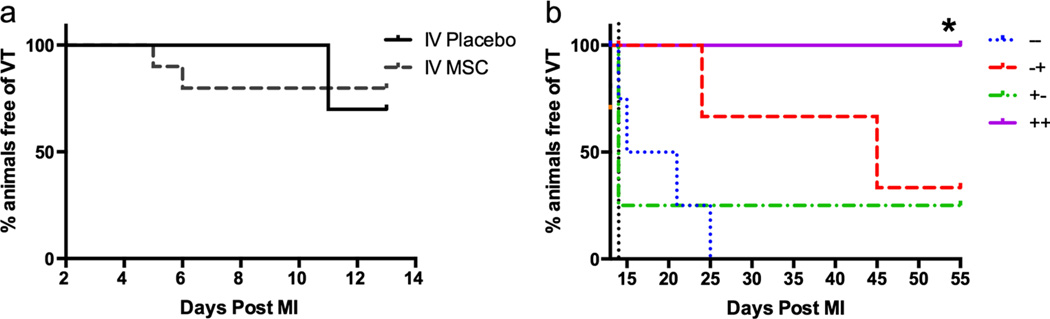
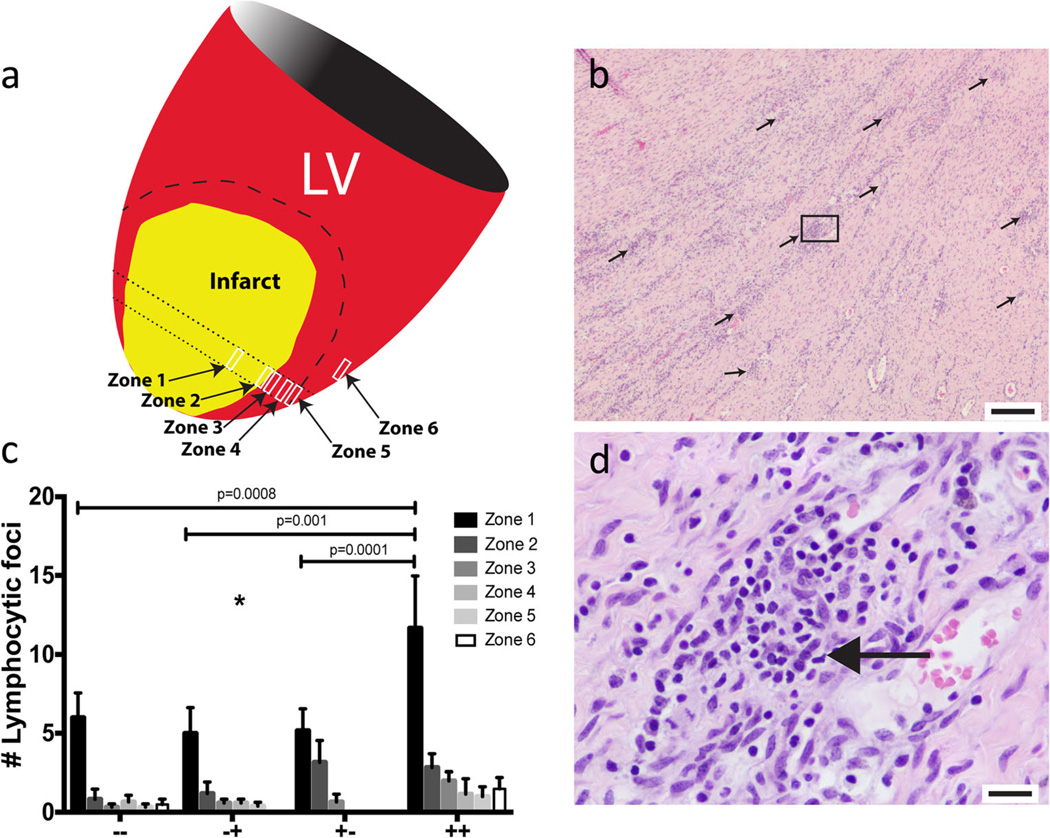
The aim of this study is to determine the effects of early intravenous (IV) infusion later followed by transendocardial (TE) injection of allogeneic mesenchymal stem cells (MSCs) following myocardial infarction (MI). Twenty-four swine underwent balloon occlusion reperfusion MI and were randomized into 4 groups: IV MSC (or placebo) infusion (post-MI day 2) and TE MSC (or placebo) injection targeting the infarct border with 2D X-ray fluoroscopy fused to 3D magnetic resonance (XFM) co-registration (post-MI day 14). Continuous ECG recording, MRI, and invasive pressure-volume analyses were performed. IV MSC plus TE MSC treated group was superior to other groups for contractility reserve (p = 0.02) and freedom from VT (p = 0.03) but had more lymphocytic foci localized to the peri-infarct region (p = 0.002). No differences were observed in post-MI remodeling parameters. IV followed by XFM targeted TE MSC therapy improves contractility reserve and suppresses VT but does not affect post-MI remodeling and may cause an immune response.
Keywords: Allogeneic; Immune response; Intravenous; Mesenchymal stem cell; Multiple dose; Myocardial infarction; Stem cell; Swine; Transendocardial.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Yeh RW, et al. Population trends in the incidence and outcomes of acute myocardial infarction. New England Journal of Medicine. 2010;362(23):2155–2165. - PubMed
-
- Goodrich AD, Hematti P. Mesenchymal stem cell therapies: the quest for fine-tuning. Experimental Dermatology. 2014;23(9):632–633. - PubMed
-
- Pittenger MF, et al. Multilineage potential of adult human mesenchymal stem cells. Science. 1999;284(5411):143–147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
