

Empirically Derived Dehydration Scoring and Decision Tree Models for Children With Diarrhea: Assessment and Internal Validation in a Prospective Cohort Study in Dhaka, Bangladesh
- PMID: 26374802
- PMCID: PMC4570015
- DOI: 10.9745/GHSP-D-15-00097
Empirically Derived Dehydration Scoring and Decision Tree Models for Children With Diarrhea: Assessment and Internal Validation in a Prospective Cohort Study in Dhaka, Bangladesh
Abstract
Introduction: Diarrhea remains one of the most common and most deadly conditions affecting children worldwide. Accurately assessing dehydration status is critical to determining treatment course, yet no clinical diagnostic models for dehydration have been empirically derived and validated for use in resource-limited settings.
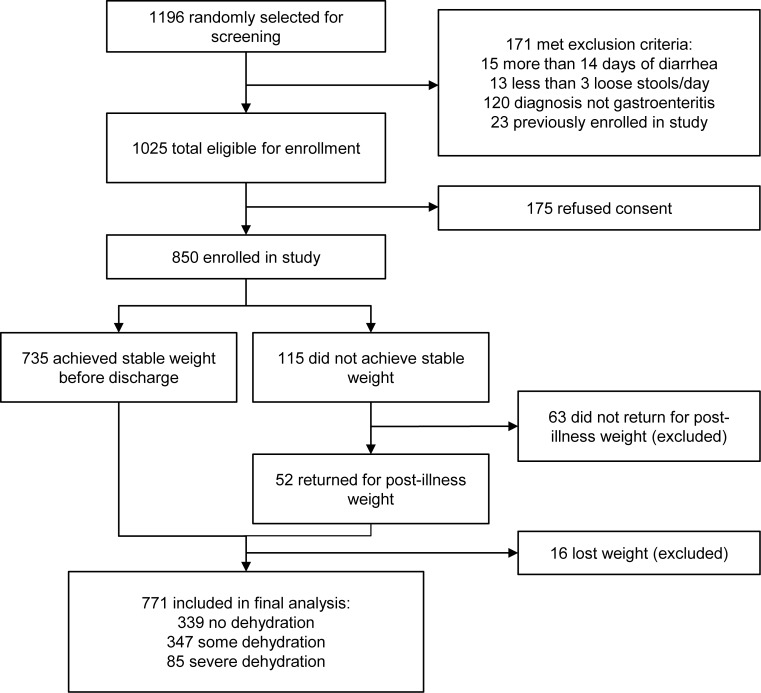
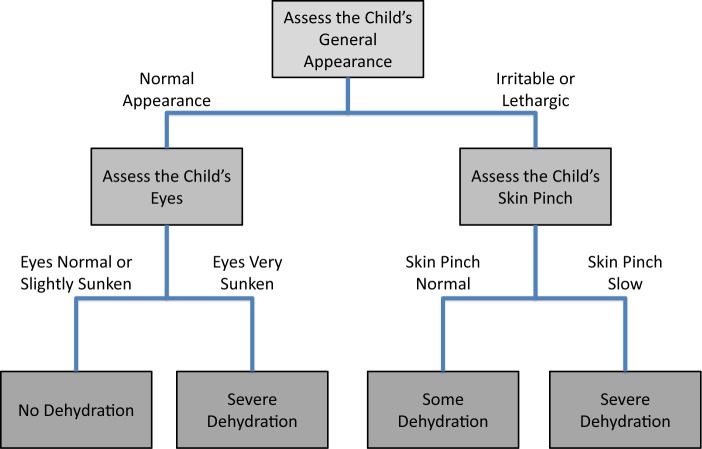
Methods: In the Dehydration: Assessing Kids Accurately (DHAKA) prospective cohort study, a random sample of children under 5 with acute diarrhea was enrolled between February and June 2014 in Bangladesh. Local nurses assessed children for clinical signs of dehydration on arrival, and then serial weights were obtained as subjects were rehydrated. For each child, the percent weight change with rehydration was used to classify subjects with severe dehydration (>9% weight change), some dehydration (3-9%), or no dehydration (<3%). Clinical variables were then entered into logistic regression and recursive partitioning models to develop the DHAKA Dehydration Score and DHAKA Dehydration Tree, respectively. Models were assessed for their accuracy using the area under their receiver operating characteristic curve (AUC) and for their reliability through repeat clinical exams. Bootstrapping was used to internally validate the models.
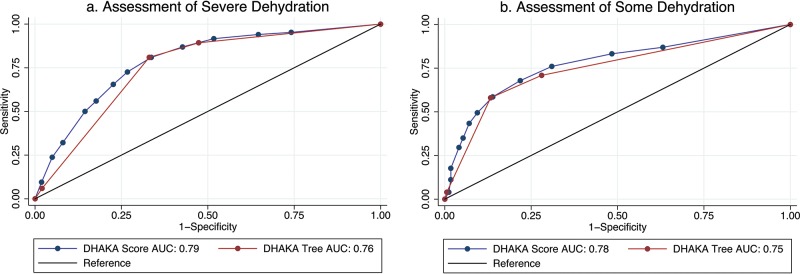
Results: A total of 850 children were enrolled, with 771 included in the final analysis. Of the 771 children included in the analysis, 11% were classified with severe dehydration, 45% with some dehydration, and 44% with no dehydration. Both the DHAKA Dehydration Score and DHAKA Dehydration Tree had significant AUCs of 0.79 (95% CI = 0.74, 0.84) and 0.76 (95% CI = 0.71, 0.80), respectively, for the diagnosis of severe dehydration. Additionally, the DHAKA Dehydration Score and DHAKA Dehydration Tree had significant positive likelihood ratios of 2.0 (95% CI = 1.8, 2.3) and 2.5 (95% CI = 2.1, 2.8), respectively, and significant negative likelihood ratios of 0.23 (95% CI = 0.13, 0.40) and 0.28 (95% CI = 0.18, 0.44), respectively, for the diagnosis of severe dehydration. Both models demonstrated 90% agreement between independent raters and good reproducibility using bootstrapping.
Conclusion: This study is the first to empirically derive and internally validate accurate and reliable clinical diagnostic models for dehydration in a resource-limited setting. After external validation, frontline providers may use these new tools to better manage acute diarrhea in children.
© Levine et al.
Figures
Similar articles
-
External validation of the DHAKA score and comparison with the current IMCI algorithm for the assessment of dehydration in children with diarrhoea: a prospective cohort study.Lancet Glob Health. 2016 Oct;4(10):e744-51. doi: 10.1016/S2214-109X(16)30150-4. Epub 2016 Aug 23. Lancet Glob Health. 2016. PMID: 27567350 Free PMC article.
-
Ultrasound Adds No Benefit to Clinical Exam for Predicting Dehydration in Children With Acute Diarrhea in a Resource-Limited Setting.J Ultrasound Med. 2019 Mar;38(3):685-693. doi: 10.1002/jum.14752. Epub 2018 Oct 5. J Ultrasound Med. 2019. PMID: 30291639
-
Derivation and Internal Validation of a Score to Predict Dehydration Severity in Patients over 5 Years with Acute Diarrhea.Am J Trop Med Hyg. 2021 Aug 16;105(5):1368-1375. doi: 10.4269/ajtmh.21-0143. Am J Trop Med Hyg. 2021. PMID: 34398821 Free PMC article.
-
Dehydration syndromes. Oral rehydration and fluid replacement.Emerg Med Clin North Am. 1991 Aug;9(3):565-88. Emerg Med Clin North Am. 1991. PMID: 2070768 Review.
-
Clinical and laboratory evaluation and management of children with vomiting, diarrhea, and dehydration.Curr Opin Pediatr. 1998 Oct;10(5):461-9. doi: 10.1097/00008480-199810000-00002. Curr Opin Pediatr. 1998. PMID: 9818241 Review.
Cited by
-
A Perspective on the Strategy for Advancing ETVAX®, An Anti-ETEC Diarrheal Disease Vaccine, into a Field Efficacy Trial in Gambian Children: Rationale, Challenges, Lessons Learned, and Future Directions.Microorganisms. 2023 Dec 31;12(1):90. doi: 10.3390/microorganisms12010090. Microorganisms. 2023. PMID: 38257916 Free PMC article.
-
Developing a Novel Mobile Health (mHealth) Tool to Improve Dehydration Assessment and Management in Patients with Acute Diarrhea in Resource-Limited Settings.R I Med J (2013). 2019 Sep 3;102(7):36-39. R I Med J (2013). 2019. PMID: 31480818 Free PMC article.
-
Rotavirus Infections: Pathophysiology, Symptoms, and Vaccination.Pathogens. 2025 May 14;14(5):480. doi: 10.3390/pathogens14050480. Pathogens. 2025. PMID: 40430800 Free PMC article. Review.
-
A machine learning approach to predicting inpatient mortality among pediatric acute gastroenteritis patients in Kenya.Learn Health Syst. 2024 Dec 26;9(2):e10478. doi: 10.1002/lrh2.10478. eCollection 2025 Apr. Learn Health Syst. 2024. PMID: 40247897 Free PMC article.
-
Assessing the performance of clinical diagnostic models for dehydration among patients with cholera and undernutrition in Bangladesh.Trop Med Int Health. 2021 Nov;26(11):1512-1525. doi: 10.1111/tmi.13675. Epub 2021 Sep 16. Trop Med Int Health. 2021. PMID: 34469615 Free PMC article.
References
-
- World Health Organization (WHO) The treatment of diarrhoea: a manual for physicians and other senior health workers. Geneva: WHO; 2005. Available from: http://www.who.int/maternal_child_adolescent/documents/9241593180/en/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical