

Influence of ejection fraction on outcomes and efficacy of spironolactone in patients with heart failure with preserved ejection fraction
- PMID: 26374849
- PMCID: PMC4751235
- DOI: 10.1093/eurheartj/ehv464
Influence of ejection fraction on outcomes and efficacy of spironolactone in patients with heart failure with preserved ejection fraction
Abstract
Aims: While mineralocorticoid receptor antagonists (MRAs) have been shown to benefit patients with reduced left ventricular ejection fraction (LVEF), spironolactone did not reduce the primary endpoint of cardiovascular death, heart failure hospitalization, or aborted cardiac arrest in patients with heart failure with preserved ejection fraction (HFpEF) in the TOPCAT trial, which enrolled patients with LVEF of 45% or greater. We utilized data from TOPCAT to assess the relationship between LVEF as well as outcomes and efficacy of spironolactone.
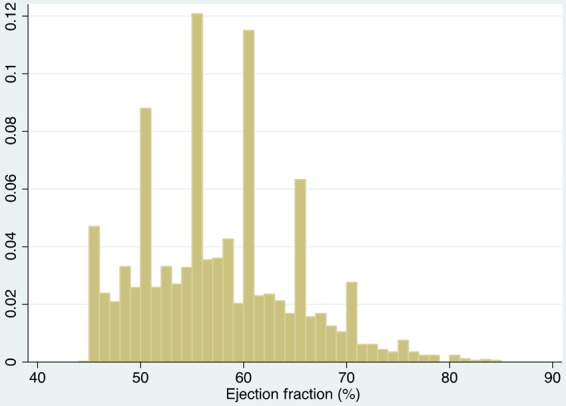
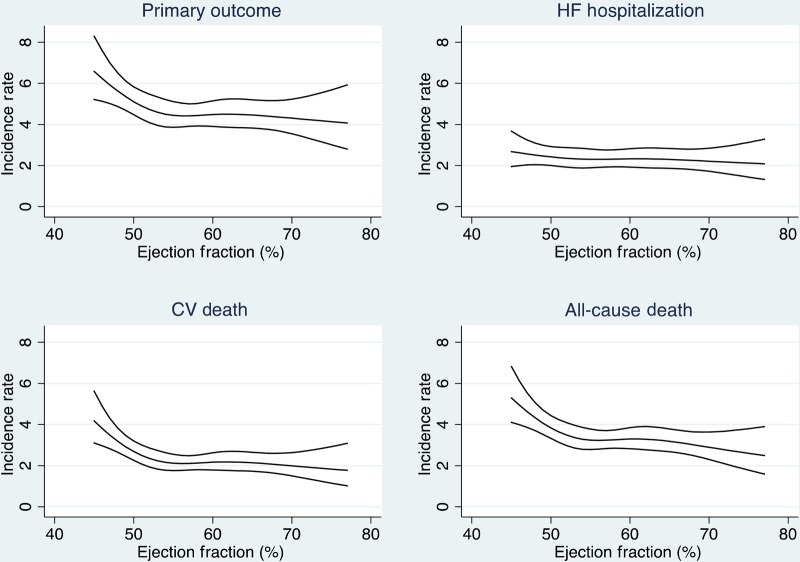
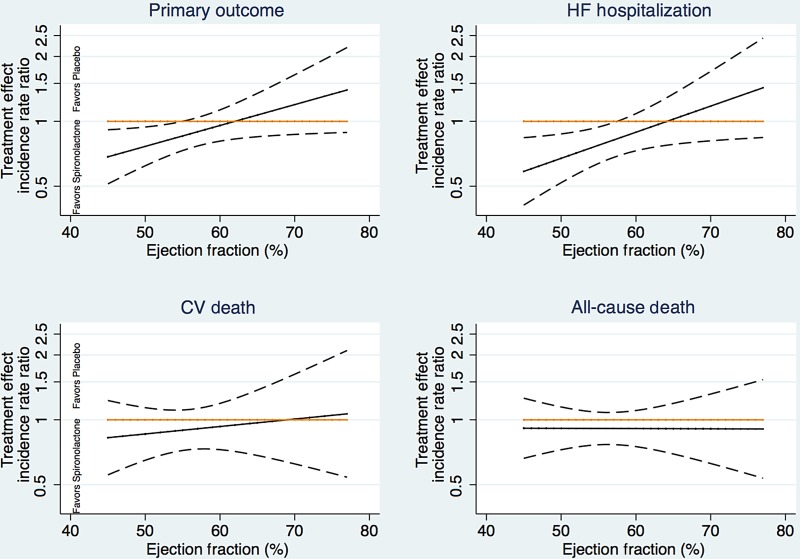
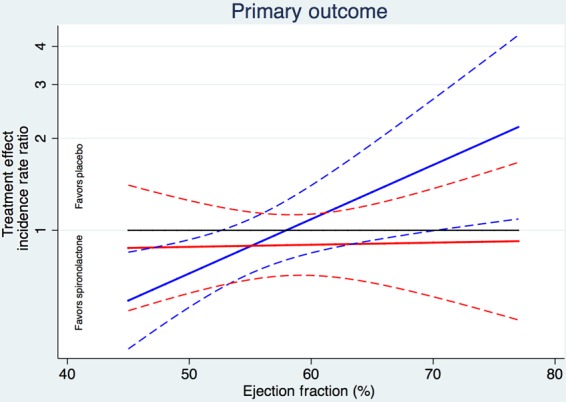
Methods and results: We assessed differences in baseline characteristics and outcomes across LVEF categories in 3444 patients with HFpEF, and determined whether LVEF modified the treatment effect of spironolactone. Ejection fraction ranged from 44 to 85%. Patients with higher ejection fraction were older, more likely to be female, less likely to have a history of myocardial infarction, and more likely to have a history of hypertension and diabetes. The incidence of the primary endpoint and cardiovascular death was highest in patients at the lower end of the ejection fraction spectrum. Ejection fraction modified the spironolactone treatment effect, particularly in the patients enrolled in the Americas, for the primary outcome (P = 0.046) and for heart failure hospitalization (P = 0.039), with stronger estimated benefits of spironolactone at the lower end of the ejection fraction spectrum with respect to the primary endpoint (LVEF <50%: HR 0.72, 95% CI 0.50, 1.05; LVEF ≥60%: HR 0.97, 95% CI 0.76, 1.23) and heart failure hospitalization (LVEF <50%: HR 0.76, 95% CI 0.46, 1.27; LVEF ≥60%: HR 0.98, 95% CI 0.74, 1.30).
Conclusion: In patients with HFpEF enrolled in TOPCAT, patient characteristics and outcomes varied substantially by LVEF. The potential efficacy of spironolactone was greatest at the lower end of the LVEF spectrum.
Clinicaltrialsgov number: NCT00094302.
Keywords: Heart failure with preserved ejection fraction; Spironolactone.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures
Comment in
-
Defining HFpEF: where do we draw the line?Eur Heart J. 2016 Feb 1;37(5):463-5. doi: 10.1093/eurheartj/ehv561. Epub 2015 Nov 3. Eur Heart J. 2016. PMID: 26530107 No abstract available.
References
-
- Butler J, Fonarow GC, Zile MR, Lam CS, Roessig L, Schelbert EB, Shah SJ, Ahmed A, Bonow RO, Cleland JG, Cody RJ, Chioncel O, Collins SP, Dunnmon P, Filippatos G, Lefkowitz MP, Marti CN, McMurray JJ, Misselwitz F, Nodari S, O'Connor C, Pfeffer MA, Pieske B, Pitt B, Rosano G, Sabbah HN, Senni M, Solomon SD, Stockbridge N, Teerlink JR, Georgiopoulou VV, Gheorghiade M. Developing therapies for heart failure with preserved ejection fraction: current state and future directions. JACC Heart Fail 2014;2:97–112. - PMC - PubMed
-
- Yusuf S, Pfeffer MA, Swedberg K, Granger C, Held P, McMurray JJV, Michelson EL, Olofsson B, Ostergren J; Charm Investigators. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARMPreserved Trial . Lancet 2003;362:777–781. - PubMed
-
- Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, Anderson S, Donovan M, Iverson E, Staiger C, Ptaszynska A; I-PRESERVE Investigators. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med 2008;359:2456–2467. - PubMed
-
- Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K, Yusuf S, Granger CB, Michelson EL, Wang D, Pocock S, Pfeffer MA; Candesartan in Heart Failure Reduction in Mortality (CHARM) Investigators. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005;112:3738–3744. - PubMed
-
- Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J 2012;33:1750–1757. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
