

Female Pattern Hair Loss: a clinical and pathophysiological review
- PMID: 26375223
- PMCID: PMC4560543
- DOI: 10.1590/abd1806-4841.20153370
Female Pattern Hair Loss: a clinical and pathophysiological review
Abstract
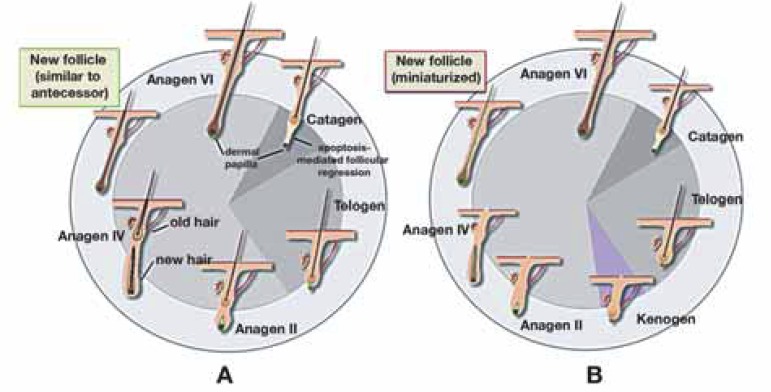
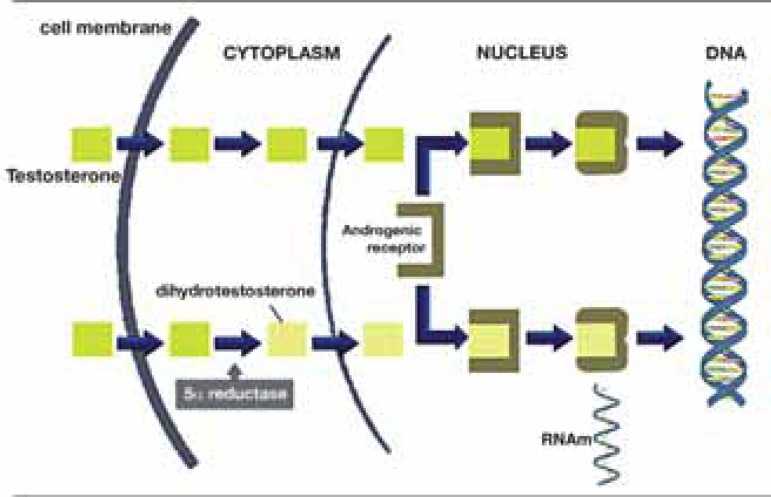
Female Pattern Hair Loss or female androgenetic alopecia is the main cause of hair loss in adult women and has a major impact on patients' quality of life. It evolves from the progressive miniaturization of follicles that lead to a subsequent decrease of the hair density, leading to a non-scarring diffuse alopecia, with characteristic clinical, dermoscopic and histological patterns. In spite of the high frequency of the disease and the relevance of its psychological impact, its pathogenesis is not yet fully understood, being influenced by genetic, hormonal and environmental factors. In addition, response to treatment is variable. In this article, authors discuss the main clinical, epidemiological and pathophysiological aspects of female pattern hair loss.
Conflict of interest statement
Conflicts of Interest: None
Figures

References
-
- Rezende JM. Linguagem médica: Alopécia, alopecia. 2011. [11 nov 2013]. Disponível em: Jmrezende.com.br. Internet. a Disponível em: http://www.jmrezende.com.br/alopecia.htm.
-
- Busca no vocabulário. Academia Brasileira de Letras; 2009. [11 nov 2013]. Disponível em: Academia.org.br. Internet. Disponível em: http://www.academia.org.br/abl/cgi/cgilua.exe/sys/start.htm?sid=23.
-
- Descritores em ciências da saúde. Biblioteca Virtual em Saúde; 2013. [11 nov 2013]. Disponível em: Decs.bvs.br. Internet. Disponível em: http://decs.bvs.br/cgi-bin/wxis1660.exe/decsserver/
-
- Plenck JJ. Doctrina de Morbis Cutaneis. Qua hi morbi in suas classes, genera et species redingtur. Vienna: Van Overbeke; 1776.
-
- Sinclair R. Winding the clock back on female androgenetic alopecia. Br J Dermatol. 2012;166:1157–1158. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical