

Do kidney stone formers have a kidney disease?
- PMID: 26376133
- PMCID: PMC4675687
- DOI: 10.1038/ki.2015.254
Do kidney stone formers have a kidney disease?
Abstract
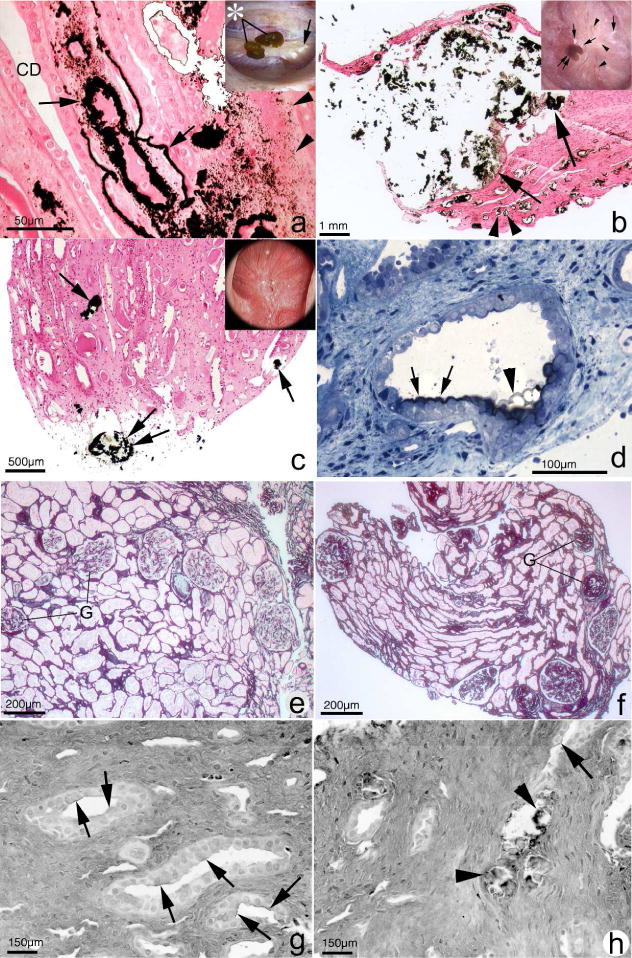
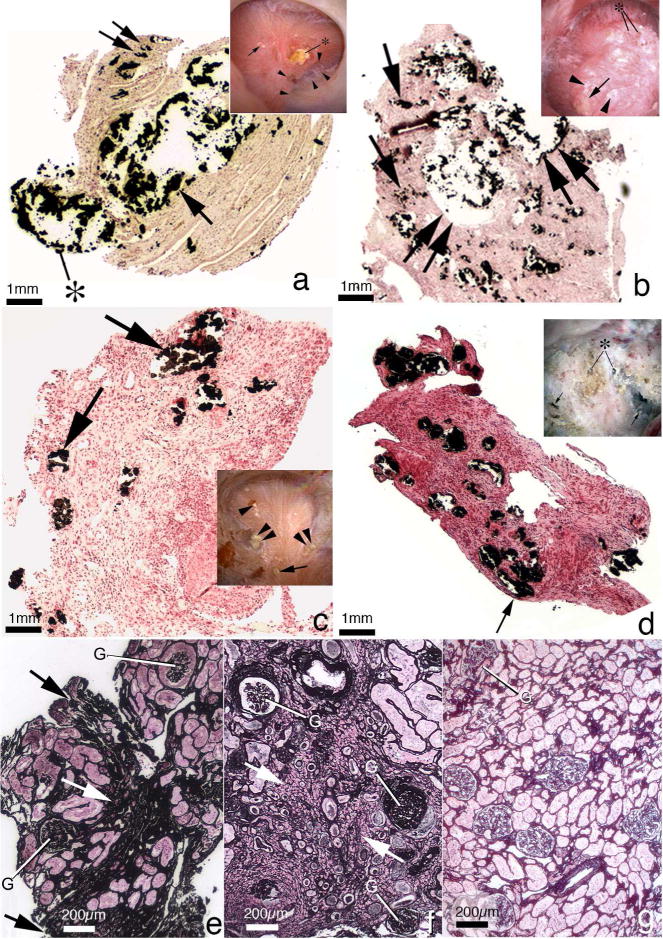
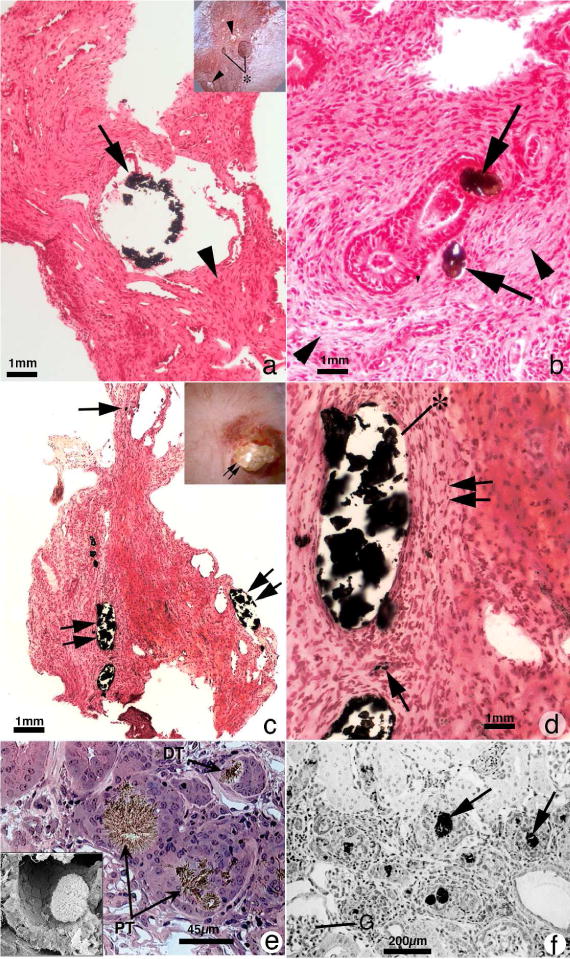
Nephrolithiasis is a highly prevalent disorder affecting approximately one in eleven people and is associated with multiple complications including hypertension, cardiovascular disease, and chronic kidney disease. Significant epidemiologic associations with chronic kidney disease and ESRD have been noted and are reviewed herein, but debate persists in the literature as to whether kidney stone formation is a pathogenic process contributing to kidney disease. Corroborating evidence supporting the presence of kidney disease in stone formers includes the variability of renal function by stone type, the positive association of stone size with renal dysfunction, the presence of markers of renal injury in the urine of even asymptomatic stone formers, and direct evidence of renal tissue injury on histopathology. Proposed pathogenic mechanisms include recurrent obstruction and comorbid conditions such as recurrent urinary tract infections and structural abnormalities. Recent work evaluating the renal histopathology of different groups of stone formers adds further granularity, suggesting variability in mechanisms of renal injury by stone type and confirming the pathogenic effects of crystal formation. Genetic abnormalities leading to stone formation including cystinuria and primary hyperoxaluria, among others, contribute to the burden of disease in the stone-forming population.
Figures
References
-
- Liu Y, Li S, Zeng Z, et al. Kidney stones and cardiovascular risk: a meta-analysis of cohort studies. Am J Kidney Dis. 2014;64(3):402–410. - PubMed
-
- Domingos F, Serra A. Metabolic syndrome: a multifaceted risk factor for kidney stones. Scand J Urol. 2014;48(5):414–419. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension. 2003;42(5):1050–1065. - PubMed
-
- Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: effects on the cardiovascular system. Circulation. 2007;116(1):85–97. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
