

Non-invasive determination by cardiovascular magnetic resonance of right ventricular-vascular coupling in children and adolescents with pulmonary hypertension
- PMID: 26376972
- PMCID: PMC4574020
- DOI: 10.1186/s12968-015-0186-1
Non-invasive determination by cardiovascular magnetic resonance of right ventricular-vascular coupling in children and adolescents with pulmonary hypertension
Abstract
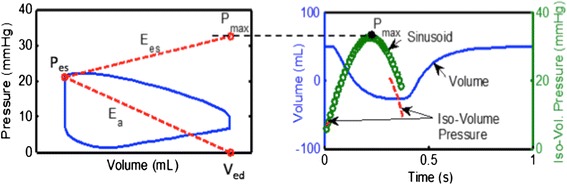
Background: Pediatric pulmonary hypertension (PH) remains a disease with high morbidity and mortality in children. Understanding ventricular-vascular coupling, a measure of how well matched the ventricular and vascular function are, may elucidate pathway leading to right heart failure. Ventricular vascular coupling ratio (VVCR), comprised of effective elastance (Ea, index of arterial load) and right ventricular maximal end-systolic elastance (Ees, index of contractility), is conventionally determined by catheterization. Here, we apply a non-invasive approach to determining VVCR in pediatric subjects with PH.
Methods: This retrospective study included PH subjects who had a cardiovascular magnetic resonance (CMR) study within 14 days of cardiac catheterization. PH was defined as mean pulmonary artery pressure (mPAP) ≥ 25 mmHg on prior or current catheterization. A non-invasive measure of VVCR was derived from CMR-only (VVCRm) and compared to VVCR estimated by catheterization-derived single beat estimation (VVCRs). Indexed pulmonary vascular resistance (PVRi) and pulmonary vascular reactivity were determined during the catheterization procedure. Pearson correlation coefficients were calculated between PVRi and VVCRm. Receiver operating characteristic (ROC) curve analysis determined the diagnostic value of VVCRm in predicting vascular reactivity.
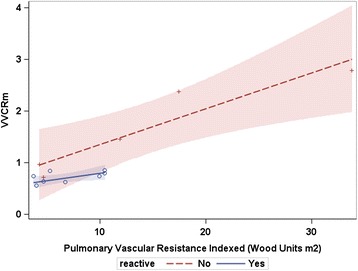
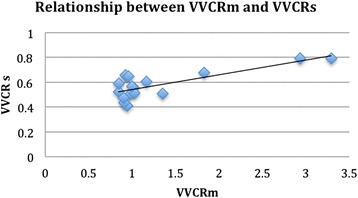
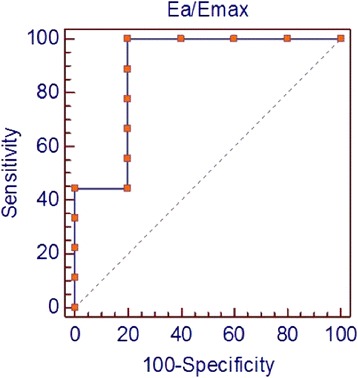
Results: Seventeen subjects (3 months-23 years; mean 11.3 ± 7.4 years) were identified between January 2009-August 2013 for inclusion with equal gender distributions. Mean mPAP was 35 mmHg ± 15 and PVRi was 8.5 Woods unit x m2 ± 7.8. VVCRm (range 0.43-2.82) increased with increasing severity as defined by PVRi (p < 0.001), and was highly correlated with PVRi (r = 0.92, 95 % CI 0.79-0.97, p < 0.0001). Regression of VVCRm and PVRi demonstrated differing lines when separated by reactivity. VVCRm was significantly correlated with VVCRs (r = 0.79, CI 0.48-0.99, p <0.0001). ROC curve analysis showed high accuracy of VVCRm in determining vascular reactivity (VVCR = 0.85 had a sensitivity of 100 % and a specificity of 80 %) with an area under the curve of 0.89 (p = 0.008).
Conclusion: Measurement of VVCRm in pediatrics is feasible. Pulmonary vascular non-reactivity may be contribute to ventricular-vascular decoupling in severe PH. Therapeutic intervention to maintain a low vascular afterload in reactive patients may preserve right ventricular functional reserve and delay the onset of RV-PA decoupling. Use of VVCRm may have significant prognostic implication.
Figures
References
-
- van Loon RL, Roofthooft MT, Hillege HL, ten Harkel AD, van Osch-Gevers M, Delhaas T, et al. Pediatric pulmonary hypertension in the Netherlands: epidemiology and characterization during the period 1991 to 2005. Circulation. 2011;124(16):1755–1764. doi: 10.1161/CIRCULATIONAHA.110.969584. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
