

Diagnostic yield of repeat sampling with immunoassay, real-time PCR, and toxigenic culture for the detection of toxigenic Clostridium difficile in an epidemic and a non-epidemic setting
- PMID: 26377204
- PMCID: PMC4655006
- DOI: 10.1007/s10096-015-2484-9
Diagnostic yield of repeat sampling with immunoassay, real-time PCR, and toxigenic culture for the detection of toxigenic Clostridium difficile in an epidemic and a non-epidemic setting
Abstract
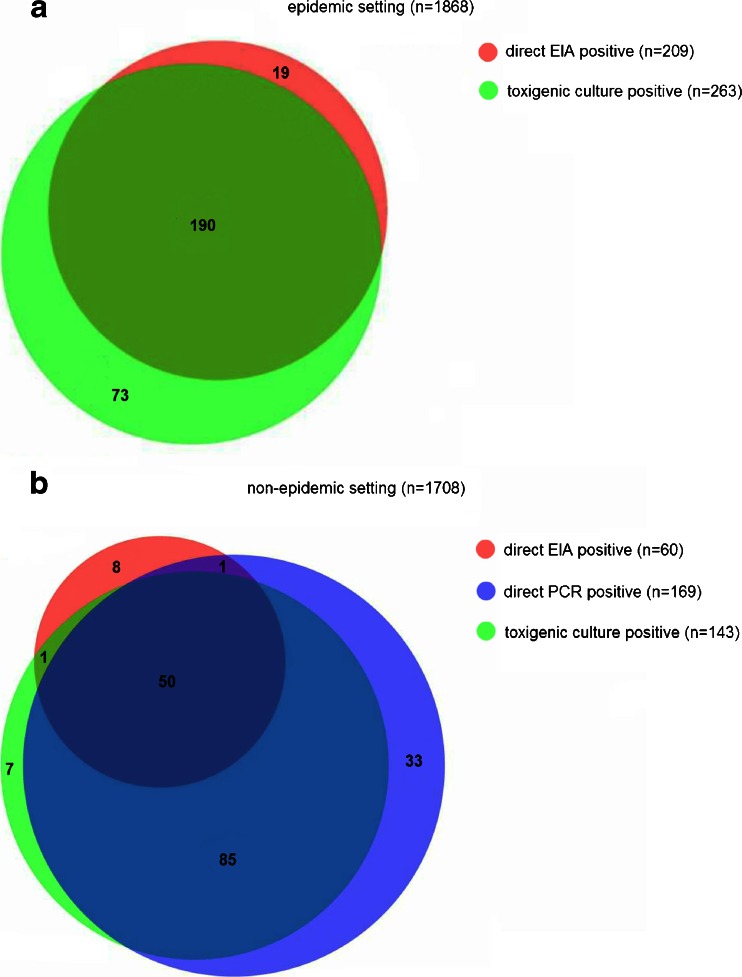
Current international guidelines lack definite conclusions regarding repeat stool sampling for the detection of toxigenic Clostridium difficile. We assessed the value of repeat sampling and compared the diagnostic yield in an epidemic to a non-epidemic setting. Consecutive fecal samples obtained during two time frames were analyzed using direct stool immunoassay toxin testing (enzyme immunoassay [EIA]), direct stool real-time PCR toxin gene testing, and toxigenic culture. Samples collected within 7 days of the initial sample were considered repeat tests. In the epidemic setting 989 patients were analyzed, and in the non-epidemic setting 1,015. In the epidemic setting 204 patients had two or more specimens included for analysis and in the non-epidemic setting 287 patients. In the epidemic setting 136 samples yielded a positive results, either by EIA or toxigenic culture; of these, 108 were positive according to EIA and 123 according to toxigenic culture. In the first test round 98 (90.7%, 95% CI 85.3 to 96.2), 114 (92.7%, 88.1 to 97.3), and 126 (92.6%, 88.3 to 97.0) positives were detected. Subsequent test rounds yielded 10 (9.3%, 3.8 to 14.7), 9 (7.3%, 2.7 to 11.9), and 10 (7.4%, 3.0 to 11.7) extra positives. In the non-epidemic setting EIA, toxigenic culture and PCR detected 33, 66, and 83 positives. The three tests combined 93 detected positives. In the first test round 30 (90.9%, 81.1 to 100.7), 63 (95.5%, 90.4 to 110.5), 76 (91.6%, 85.6 to 97.5), and 87 (93.5%, 88.6 to 98.5) positives were detected. Subsequent test rounds yielded 3 (9.1%, -0.7 to 18.9), 3 (4.5%, -0.5 to 9.6), 7 (8.4%, 2.5 to 14.4), and 6 (6.5%, 1.5 to 11.4) extra positives. In conclusion, repeat testing resulted in 4.5% to 9.3% extra positives. No significant difference between the settings studied could be demonstrated. Repeat sampling and multimodality testing may be chosen in an outbreak situation to detect all cases, effectively controlling nosocomial spread.
Figures
Similar articles
-
Evaluation of the illumigene C. difficile assay for toxigenic Clostridium difficile detection: a prospective study of 302 consecutive clinical fecal samples.Diagn Microbiol Infect Dis. 2014 Nov;80(3):177-80. doi: 10.1016/j.diagmicrobio.2014.08.014. Epub 2014 Sep 2. Diagn Microbiol Infect Dis. 2014. PMID: 25241189
-
Two-step glutamate dehydrogenase antigen real-time polymerase chain reaction assay for detection of toxigenic Clostridium difficile.J Hosp Infect. 2010 Jan;74(1):48-54. doi: 10.1016/j.jhin.2009.08.014. Epub 2009 Nov 8. J Hosp Infect. 2010. PMID: 19900734
-
Clostridium difficile infection diagnostics - evaluation of the C. DIFF Quik Chek Complete assay, a rapid enzyme immunoassay for detection of toxigenic C. difficile in clinical stool samples.APMIS. 2016 Nov;124(11):1016-1020. doi: 10.1111/apm.12595. Epub 2016 Sep 20. APMIS. 2016. PMID: 27651167
-
Tests for the diagnosis of Clostridium difficile infection: the next generation.Anaerobe. 2011 Aug;17(4):170-4. doi: 10.1016/j.anaerobe.2011.01.002. Epub 2011 Mar 3. Anaerobe. 2011. PMID: 21376826 Review.
-
Laboratory diagnosis of Clostridium difficile-associated diarrhoea: a plea for culture.J Med Microbiol. 2005 Feb;54(Pt 2):187-191. doi: 10.1099/jmm.0.45844-0. J Med Microbiol. 2005. PMID: 15673515 Review.
Cited by
-
Clostridium difficile infections in young infants: Case presentations and literature review.IDCases. 2017 Jul 24;10:7-11. doi: 10.1016/j.idcr.2017.07.005. eCollection 2017. IDCases. 2017. PMID: 28791215 Free PMC article.
-
Implementing a Clostridium difficile testing algorithm and its effect on isolation duration and treatment initiation: a pre- and post-implementation study.Eur J Clin Microbiol Infect Dis. 2020 Jun;39(6):1071-1076. doi: 10.1007/s10096-020-03823-w. Epub 2020 Jan 23. Eur J Clin Microbiol Infect Dis. 2020. PMID: 31970532 Free PMC article.
-
The Role of Diagnostic Stewardship in Clostridioides difficile Testing: Challenges and Opportunities.Curr Infect Dis Rep. 2020 Mar;22(3):7. doi: 10.1007/s11908-020-0715-4. Epub 2020 Feb 17. Curr Infect Dis Rep. 2020. PMID: 33762897 Free PMC article.
-
Diagnostic Guidance for C. difficile Infections.Adv Exp Med Biol. 2024;1435:33-56. doi: 10.1007/978-3-031-42108-2_3. Adv Exp Med Biol. 2024. PMID: 38175470
-
An Outbreak of Clostridium difficile Ribotype 027 Associated with Length of Stay in the Intensive Care Unit and Use of Selective Decontamination of the Digestive Tract: A Case Control Study.PLoS One. 2016 Aug 17;11(8):e0160778. doi: 10.1371/journal.pone.0160778. eCollection 2016. PLoS One. 2016. PMID: 27533048 Free PMC article.
References
-
- Peterson LR, Manson RU, Paule SM, Hacek DM, Robicsek A, Thomson RB, Jr, Kaul KL. Detection of toxigenic Clostridium difficile in stool samples by real-time polymerase chain reaction for the diagnosis of C. difficile-associated diarrhea. Clin Infect Dis. 2007;45:1152–1160. doi: 10.1086/522185. - DOI - PubMed
-
- Alcala L, Marin M, Madrid M, Dominguez-Garcia E, Catalan P, Pelaez MT, Sanchez-Somolinos M, Bouza E. Comparison of ImmunoCard Toxins A&B and the new semiautomated Vidas Clostridium difficile Toxin A&B tests for diagnosis of C. difficile infection. J Clin Microbiol. 2010;48:1014–1015. doi: 10.1128/JCM.01642-09. - DOI - PMC - PubMed
-
- Stamper PD, Alcabasa R, Aird D, Babiker W, Wehrlin J, Ikpeama I, Carroll KC. Comparison of a commercial real-time PCR assay for tcdB detection to a cell culture cytotoxicity assay and toxigenic culture for direct detection of toxin-producing Clostridium difficile in clinical samples. J Clin Microbiol. 2009;47:373–378. doi: 10.1128/JCM.01613-08. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
