

Four-dimensional flow magnetic resonance imaging-based characterization of aortic morphometry and haemodynamics: impact of age, aortic diameter, and valve morphology
- PMID: 26377908
- PMCID: PMC4955292
- DOI: 10.1093/ehjci/jev228
Four-dimensional flow magnetic resonance imaging-based characterization of aortic morphometry and haemodynamics: impact of age, aortic diameter, and valve morphology
Abstract
Aims: Four-dimensional (4D) flow magnetic resonance imaging (MRI) was employed for the simultaneous assessment of morphometry and flow parameters along the thoracic aorta to investigate associations between flow, age, aorta diameter, and aortic valve morphology.
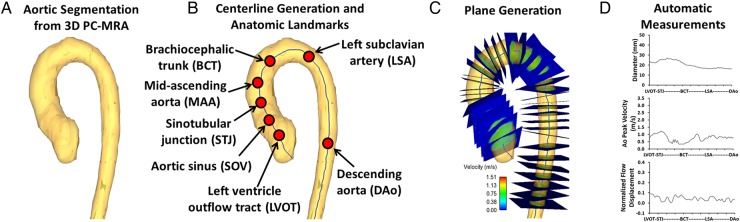
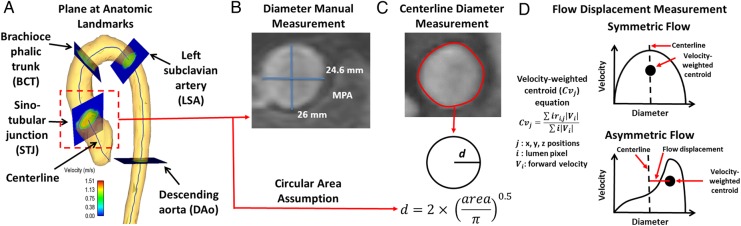
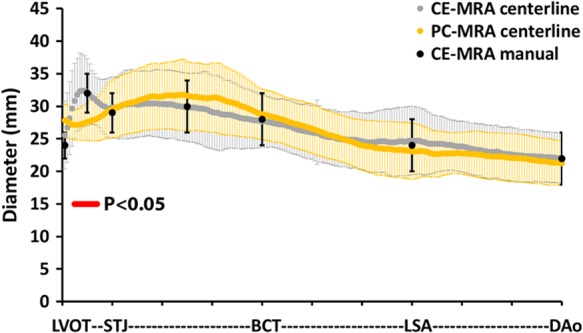
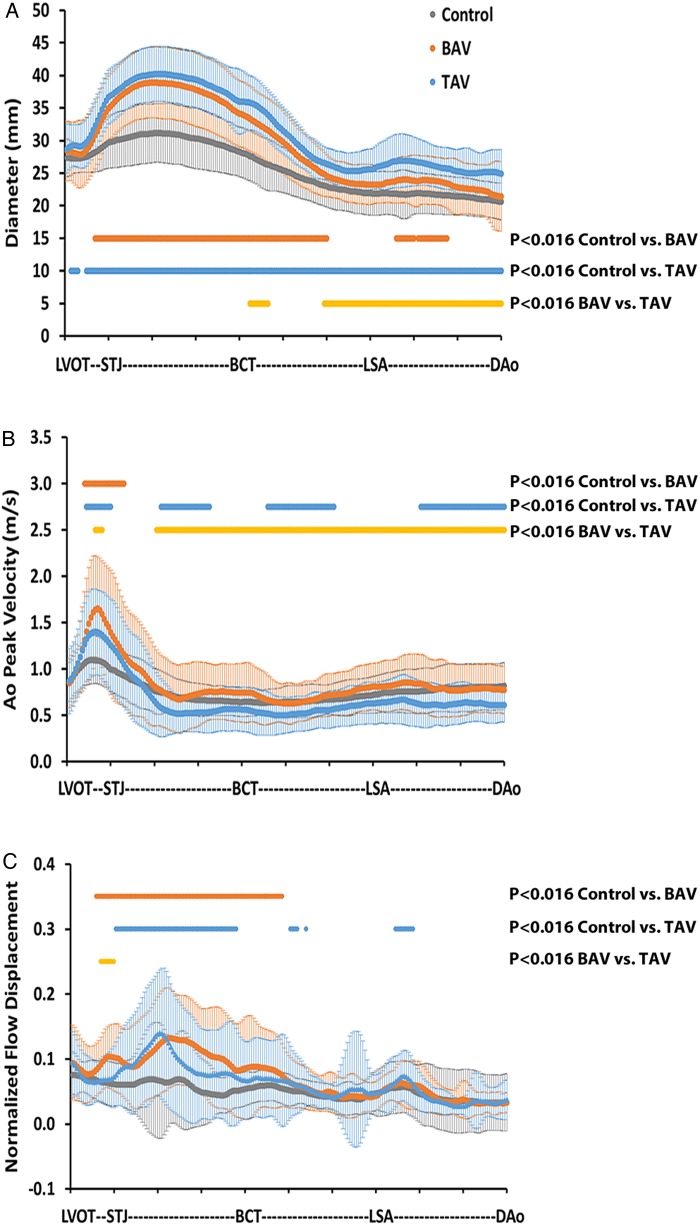
Methods and results: One hundred and sixty-five subjects, 65 controls, 50 patients with bicuspid aortic valve (BAV), and 50 patients with a dilated aorta, and a tricuspid aortic valve (TAV) underwent 4D flow MRI. Following 3D segmentation of the aorta, a vessel centreline was calculated and used to extract aorta diameter, peak systolic velocity, and normalized systolic flow displacement. Validation of 4D flow MRI-based morphometric measurements compared with manual diameter measurements from standard contrast-enhanced MR angiography in 20 controls showed good agreement (mean difference = 0.4 mm, limits of agreement = ±1.31 mm) except at the sinus of valsalva. BAV showed significant differences in average peak velocity (PV; P < 0.016) compared with TAV and controls between the left ventricle outflow tract to sino-tubular junction (BAV: 1.3 ± 0.3 m/s; TAV: 1.2 ± 0.2 m/s; controls: 1.0 ± 0.1 m/s) and the ascending aorta for average normalized flow displacement (BAV: 0.11 ± 0.02; TAV: 0.09 ± 0.02; controls: 0.06 ± 0.01, P < 0.016) despite similar average aortic dimensions for BAV (37 ± 1 mm) and TAV (39 ± 1 mm). Multivariate linear regression showed a significant correlation of maximal aortic diameter to age, PV, and normalized flow displacement (R(2) = 0.413, P < 0.001).
Conclusion: A single acquisition of 4D flow MRI characterized local morphological and haemodynamic differences between groups along the aorta. BAV showed altered haemodynamics when compared with TAV in spite of having similar aorta dimensions. Maximal aorta diameter was associated with age, PV, and normalized flow displacement.
Keywords: Aortic diseases; Haemodynamics; Magnetic resonance imaging.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures
Similar articles
-
Haemodynamic outcome at four-dimensional flow magnetic resonance imaging following valve-sparing aortic root replacement with tricuspid and bicuspid valve morphology.Eur J Cardiothorac Surg. 2014 May;45(5):818-25. doi: 10.1093/ejcts/ezt526. Epub 2013 Dec 6. Eur J Cardiothorac Surg. 2014. PMID: 24317086 Free PMC article.
-
Valve mediated hemodynamics and their association with distal ascending aortic diameter in bicuspid aortic valve subjects.J Magn Reson Imaging. 2018 Jan;47(1):246-254. doi: 10.1002/jmri.25719. Epub 2017 Apr 8. J Magn Reson Imaging. 2018. PMID: 28390180 Free PMC article.
-
Interval changes in aortic peak velocity and wall shear stress in patients with bicuspid aortic valve disease.Int J Cardiovasc Imaging. 2019 Oct;35(10):1925-1934. doi: 10.1007/s10554-019-01632-7. Epub 2019 May 29. Int J Cardiovasc Imaging. 2019. PMID: 31144256 Free PMC article.
-
Multimodality imaging in bicuspid aortic valve.Prog Cardiovasc Dis. 2020 Jul-Aug;63(4):442-451. doi: 10.1016/j.pcad.2020.06.003. Epub 2020 Jun 9. Prog Cardiovasc Dis. 2020. PMID: 32531300 Review.
-
Functional assessment of thoracic aortic aneurysms - the future of risk prediction?Br Med Bull. 2017 Jan 1;121(1):61-71. doi: 10.1093/bmb/ldw049. Br Med Bull. 2017. PMID: 27989994 Free PMC article. Review.
Cited by
-
Hemodynamic Profiles Before and After Surgery in Bicuspid Aortic Valve Disease-A Systematic Review of the Literature.Front Cardiovasc Med. 2021 Mar 24;8:629227. doi: 10.3389/fcvm.2021.629227. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33842561 Free PMC article. Review.
-
Reproducibility and Changes in Vena Caval Blood Flow by Using 4D Flow MRI in Pulmonary Emphysema and Chronic Obstructive Pulmonary Disease (COPD): The Multi-Ethnic Study of Atherosclerosis (MESA) COPD Substudy.Radiology. 2019 Sep;292(3):585-594. doi: 10.1148/radiol.2019182143. Epub 2019 Jul 23. Radiology. 2019. PMID: 31335282 Free PMC article.
-
Clinical Applications of MRA 4D-Flow.Curr Treat Options Cardiovasc Med. 2019 Sep 10;21(10):58. doi: 10.1007/s11936-019-0758-8. Curr Treat Options Cardiovasc Med. 2019. PMID: 31506869 Review.
-
Volumetric quantification of absolute local normalized helicity in patients with bicuspid aortic valve and aortic dilatation.Magn Reson Med. 2017 Aug;78(2):689-701. doi: 10.1002/mrm.26387. Epub 2016 Aug 19. Magn Reson Med. 2017. PMID: 27539068 Free PMC article.
-
Implications of Bicuspid Aortic Valve Disease and Aortic Stenosis/Insufficiency as Risk Factors for Thoracic Aortic Aneurysm.Rev Cardiovasc Med. 2023 Jun 19;24(6):178. doi: 10.31083/j.rcm2406178. eCollection 2023 Jun. Rev Cardiovasc Med. 2023. PMID: 39077527 Free PMC article. Review.
References
-
- Verma S, Siu SC. Aortic dilatation in patients with bicuspid aortic valve. N Engl J Med 2014;370:1920–9. - PubMed
-
- Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggbrech H et al. . ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J 2014;35:2873–926. - PubMed
-
- Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Barón-Esquivias G, Baumgartner H et al. . Guidelines on the management of valvular heart disease. Eur Heart J 2012;33:2451–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
