

Tubal ligation and ovarian cancer risk in a large cohort: Substantial variation by histological type
- PMID: 26378908
- PMCID: PMC4832307
- DOI: 10.1002/ijc.29856
Tubal ligation and ovarian cancer risk in a large cohort: Substantial variation by histological type
Abstract
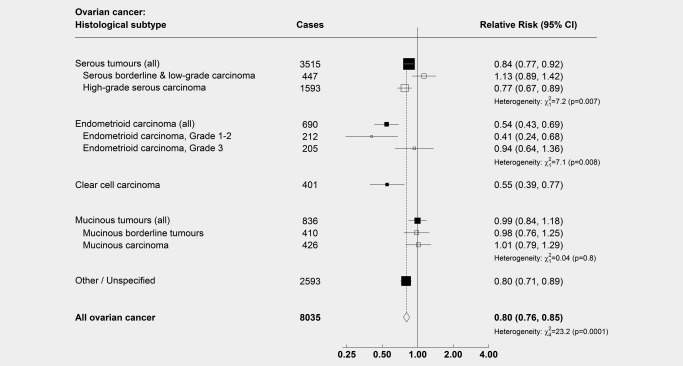
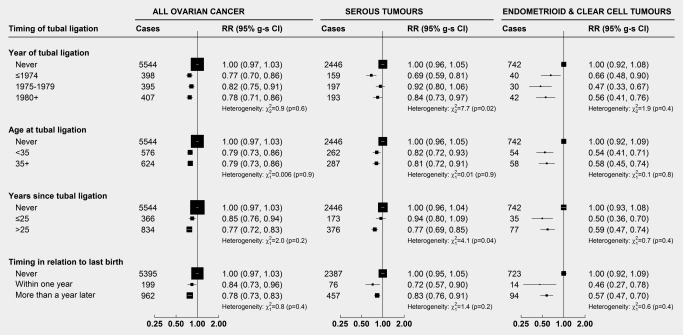
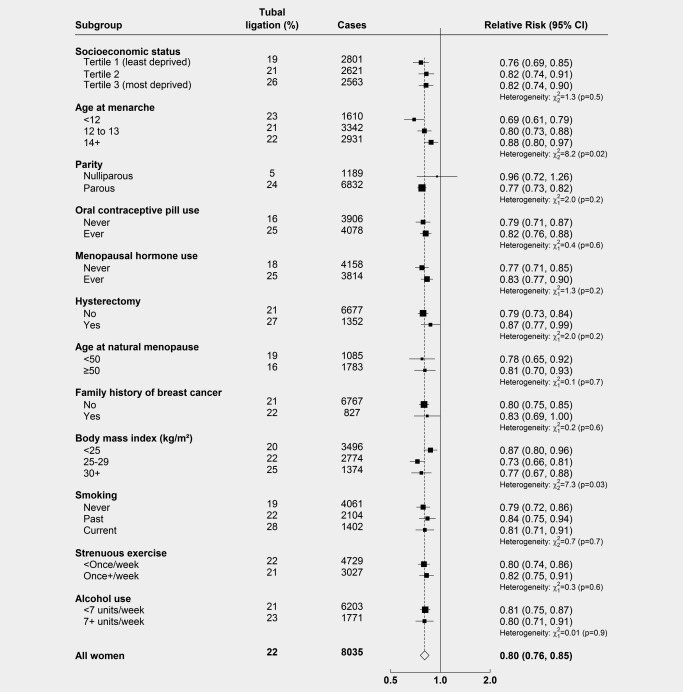
Histopathological and molecular studies suggest that different histological subtypes (histotypes) of ovarian cancer have different aetiologies. Few studies have been large enough to explore reliably the effect of tubal ligation (sterilization), which has been associated with a reduced overall risk of ovarian cancer, on different tumour histotypes. In a prospective study of 1.1 million UK women without prior cancer or bilateral oophorectomy, 8,035 ovarian cancers occurred during mean follow-up of 13.8 years. Using a Cox proportional hazards model, we estimated adjusted relative risks of ovarian cancer associated with tubal ligation. Overall, there was substantial heterogeneity in tumour risk associated with tubal ligation for the four main histotypes, serous, endometrioid, mucinous and clear cell (heterogeneity: p < 0.0001). For serous tumours, the most common histotype (n = 3,515), risks differed significantly between high-grade (RR: 0.77, 95% CI: 0.67-0.89) and low-grade tumours (RR: 1.13, 95% CI: 0.89-1.42); heterogeneity: p = 0.007. Relative risks were almost halved for endometrioid (n = 690, RR: 0.54, 95% CI: 0.43-0.69) and clear cell tumours (n = 401, RR: 0.55, 95% CI: 0.39-0.77), but there was no association between tubal ligation and mucinous tumours (n = 836, RR: 0.99, 95% CI: 0.84-1.18). For the main tumour histotypes we found little variation of risk by timing of tubal ligation. The significant differences by tumour histotype are unlikely to be due to confounding and are consistent with hypotheses that high-grade and low-grade serous tumours have different origins, and that some endometrioid and clear cell tumours might arise from cells and/or carcinogens travelling through the fallopian tubes.
Keywords: histological subtypes; histotype; ovarian cancer; sterilization; tubal ligation.
© 2015 The Authors International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Figures
References
-
- Forman D, Bray F, Brewster D, et al. eds. Cancer incidence in five continents, vol. 10 Lyon: International Agency for Research on Cancer (IARC Scientific Publication No. 164.ed.), 2014.
-
- Prat J. Ovarian carcinomas: five distinct diseases with different origins, genetic alterations, and clinicopathological features. Virchows Arch 2012;460:237–49. - PubMed
-
- Kurman RJ, Carcangiu ML, Herrington CS, et al., eds. WHO classification of tumours of female reproductive organs, 4th edn Lyon: IARC, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
