

Percutaneous Coronary Intervention Utilization and Appropriateness across the United States
- PMID: 26379053
- PMCID: PMC4575022
- DOI: 10.1371/journal.pone.0138251
Percutaneous Coronary Intervention Utilization and Appropriateness across the United States
Abstract
Background: Substantial geographic variation exists in percutaneous coronary intervention (PCI) use across the United States. It is unclear the extent to which high PCI utilization can be explained by PCI for inappropriate indications. The objective of this study was to examine the relationship between PCI rates across regional healthcare markets utilizing hospital referral regions (HRRs) and PCI appropriateness.
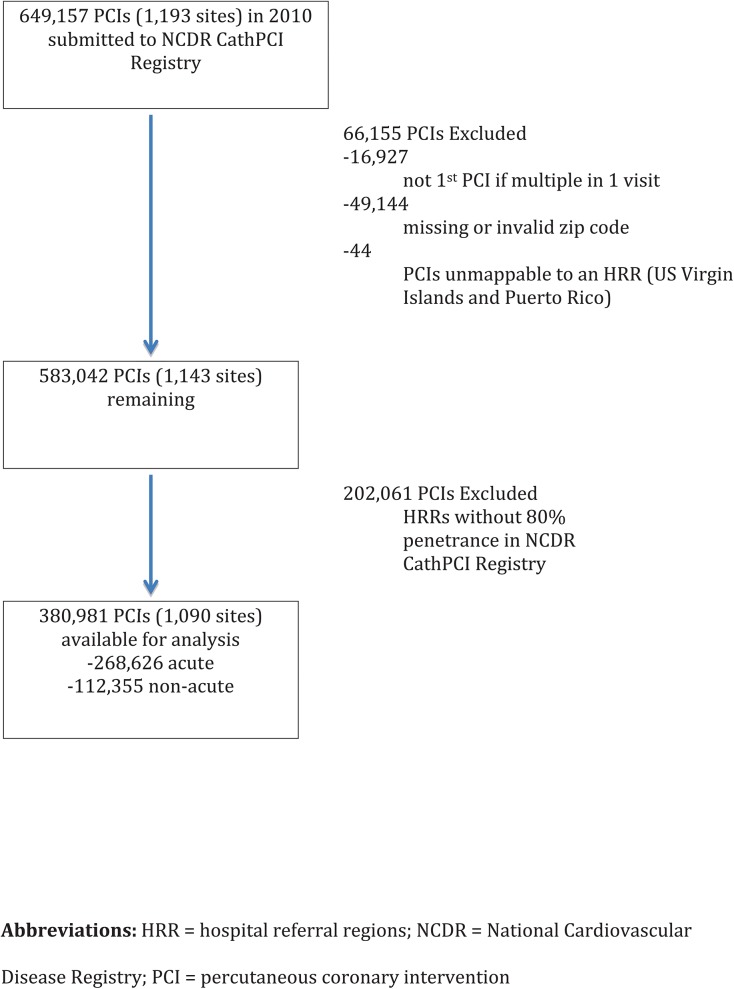
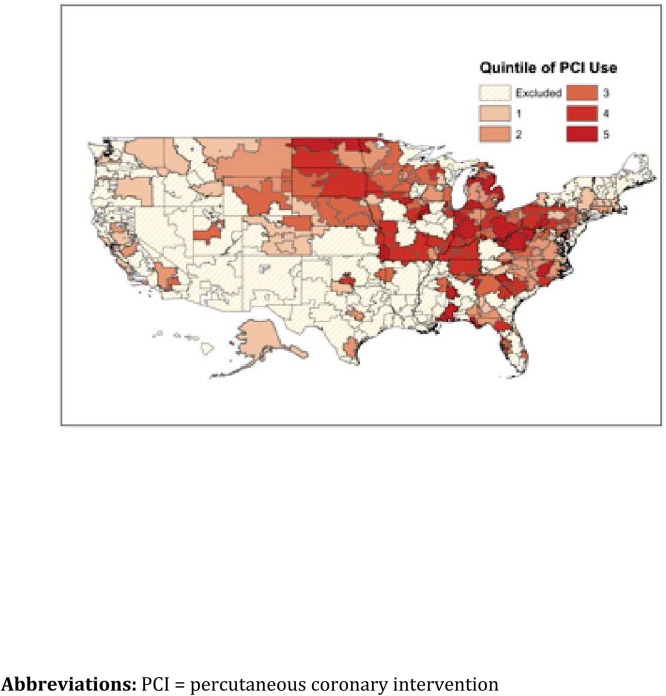
Methods: The number of PCI procedures in each HRR was obtained from the 2010 100% Medicare limited data set. HRRs were divided into quintiles of PCI utilization with increasing rates of utilization progressing to quintile 5. NCDR CathPCI Registry® data were used to evaluate patient characteristics, appropriate use criteria (AUC), and outcomes across the HRR quintiles defined by PCI utilization with the study population restricted to HRRs where ≥ 80% of the PCIs were performed at institutions participating in the registry. PCI appropriateness was defined using 2012 AUC by the American College of Cardiology (ACC)/American Heart Association (AHA)/The Society for Cardiovascular Angiography and Interventions (SCAI).
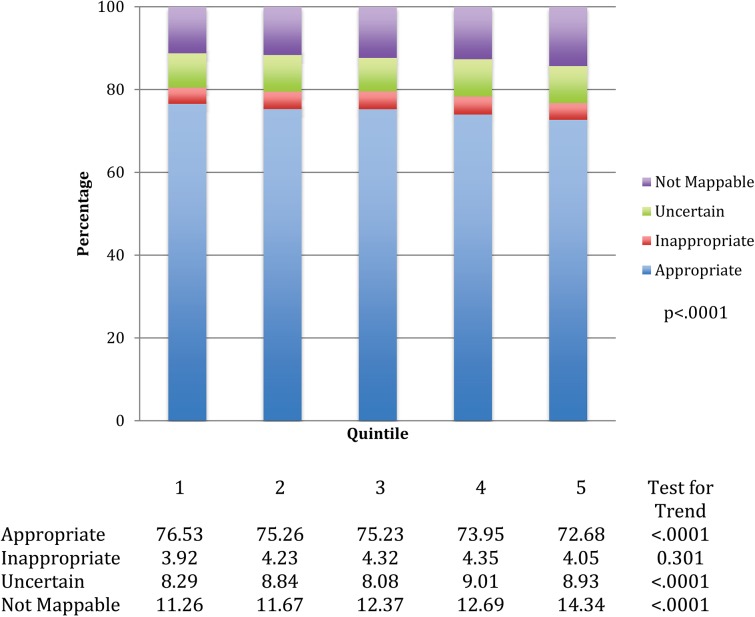
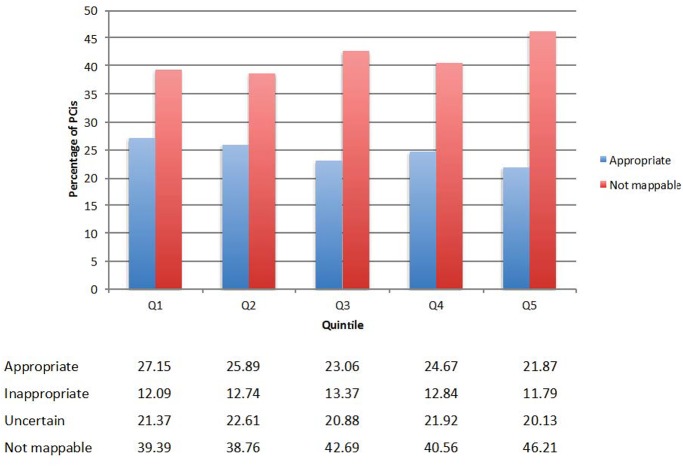
Results: Our study cohort comprised of 380,981 patients treated at 178 HRRs. Mean PCI rates per 1,000 increased from 4.6 in Quintile 1 to 10.8 in Quintile 5. The proportion of non-acute PCIs was 27.7% in Quintile 1 increasing to 30.7% in Quintile 5. Significant variation (p < 0.001) existed across the quintiles in the categorization of appropriateness across HRRs of utilization with more appropriate PCI in lower utilization areas (Appropriate: Q1, 76.53%, Q2, 75.326%, Q3, 75.23%, Q4, 73.95%, Q5, 72.768%; Inappropriate: Q1 3.92%, Q2 4.23%, Q3 4.32%, Q4 4.35%, Q5 4.05%; Uncertain: Q1 8.29%, Q2 8.84%, Q3 8.08%, Q4 9.01%, Q5 8.93%; Not Mappable: Q1 11.26%, Q2 11.67%, Q3 12.37%, Q4 12.69%, Q5 14.34%). There was no difference in risk-adjusted mortality across quintiles of PCI utilization.
Conclusions: Geographic regions with lower PCI rates have a higher proportion of PCIs performed for appropriate indications. Areas that perform more PCIs also appear to perform more elective PCI and many could not be mapped by the AUC.
Conflict of interest statement
Figures
References
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Journal of the American College of Cardiology 2011;58:e44–122. 10.1016/j.jacc.2011.08.007 - DOI - PubMed
-
- Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: a report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. Journal of the American College of Cardiology 2009;53:530–553. 10.1016/j.jacc.2008.10.005 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
