

Artifacts and pitfalls in shoulder magnetic resonance imaging
- PMID: 26379323
- PMCID: PMC4567363
- DOI: 10.1590/0100-3984.2013.0006
Artifacts and pitfalls in shoulder magnetic resonance imaging
Abstract
Magnetic resonance imaging has revolutionized the diagnosis of shoulder lesions, in many cases becoming the method of choice. However, anatomical variations, artifacts and the particularity of the method may be a source of pitfalls, especially for less experienced radiologists. In order to avoid false-positive and false-negative results, the authors carried out a compilation of imaging findings that may simulate injury. It is the authors' intention to provide a useful, consistent and comprehensive reference for both beginner residents and skilled radiologists who work with musculoskeletal magnetic resonance imaging, allowing for them to develop more precise reports and helping them to avoid making mistakes.
A ressonância magnética revolucionou o diagnóstico de lesões do ombro, tornando-se, em muitos casos, o método de escolha. No entanto, as variações anatômicas, artefatos e particularidade do método podem ser fonte de armadilhas, especialmente para radiologistas menos experientes. Para evitar resultados falso-positivos e falso-negativos, foi realizada uma compilação de achados de imagem que podem simular lesões. Pretendemos ser uma referência útil, consistente e abrangente para os residentes iniciantes e radiologistas qualificados que trabalham com ressonância magnética musculoesquelética, a fim de desenvolver relatórios mais precisos e ajudá-los a evitar erros.
Keywords: Artifacts; Magnetic resonance imaging; Musculoskeletal; Pitfalls; Shoulder.
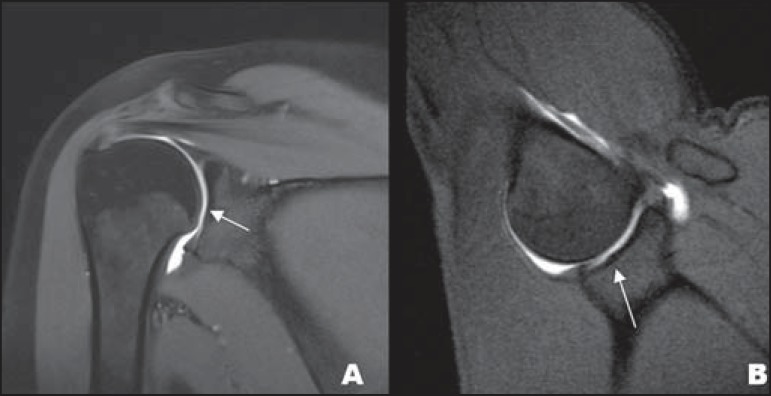
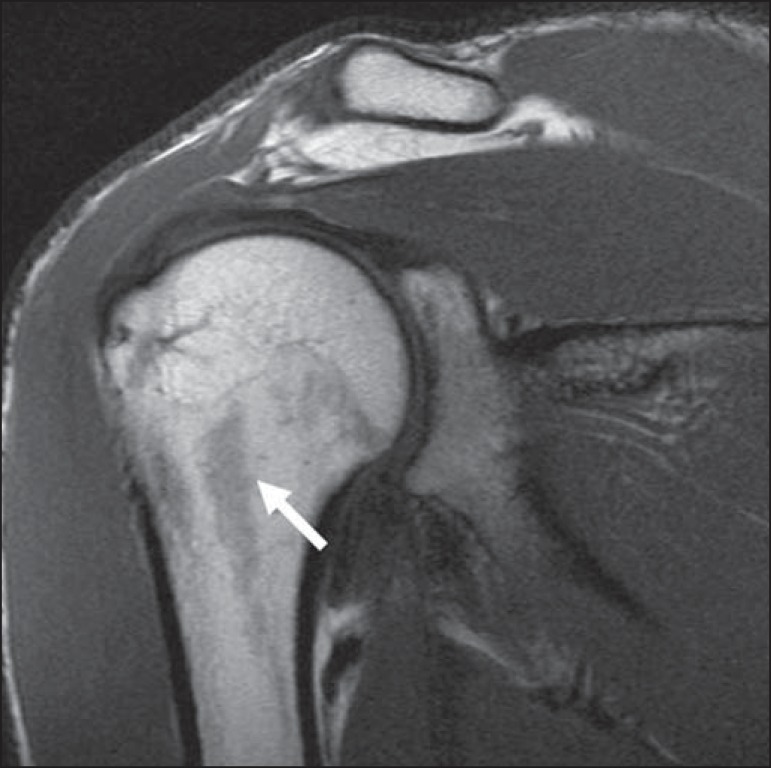
Figures
References
-
- Pal GP, Bhatt RH, Patel VS. Relationship between the tendon of the long head of biceps brachii and the glenoidal labrum in humans. Anat Rec. 1991;229:278–280. - PubMed
-
- Vangsness CT, Jr, Jorgenson SS, Watson T, et al. The origin of the long head of the biceps from the scapula and glenoid labrum. An anatomical study of 100 shoulders. J Bone Joint Surg Br. 1994;76:951–954. - PubMed
-
- Fitzpatrick D, Walz DM. Shoulder MR imaging normal variants and imaging artifacts. Magn Reson Imaging Clin N Am. 2010;18:615–632. - PubMed
-
- MacDonald PB. Congenital anomaly of the biceps tendon and anatomy within the shoulder joint. Arthroscopy. 1998;14:741–742. - PubMed
-
- Yeh L, Pedowitz R, Kwak S, et al. Intracapsular origin of the long head of the biceps tendon. Skeletal Radiol. 1999;28:178–181. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources