

Are the Two Human Papillomavirus Vaccines Really Similar? A Systematic Review of Available Evidence: Efficacy of the Two Vaccines against HPV
- PMID: 26380321
- PMCID: PMC4562171
- DOI: 10.1155/2015/435141
Are the Two Human Papillomavirus Vaccines Really Similar? A Systematic Review of Available Evidence: Efficacy of the Two Vaccines against HPV
Erratum in
-
Corrigendum to "Are the Two Human Papillomavirus Vaccines Really Similar? A Systematic Review of Available Evidence: Efficacy of the Two Vaccines against HPV".J Immunol Res. 2017;2017:4583487. doi: 10.1155/2017/4583487. Epub 2017 May 30. J Immunol Res. 2017. PMID: 28744473 Free PMC article.
Abstract
Background: When the bivalent and the quadrivalent HPV vaccines were marketed they were presented as having comparable efficacy against cervical cancer. Differences between the vaccines are HPV types included and formulation of the adjuvant.
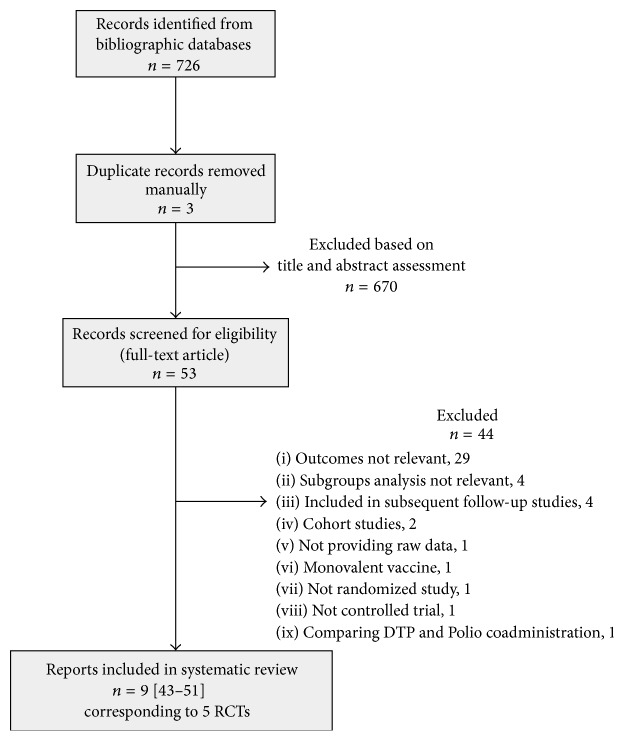
Method: A systematic review was conducted to assess the efficacy of the two vaccines against cervical cancer. Outcomes considered were CIN2+, CIN3+, and AIS.
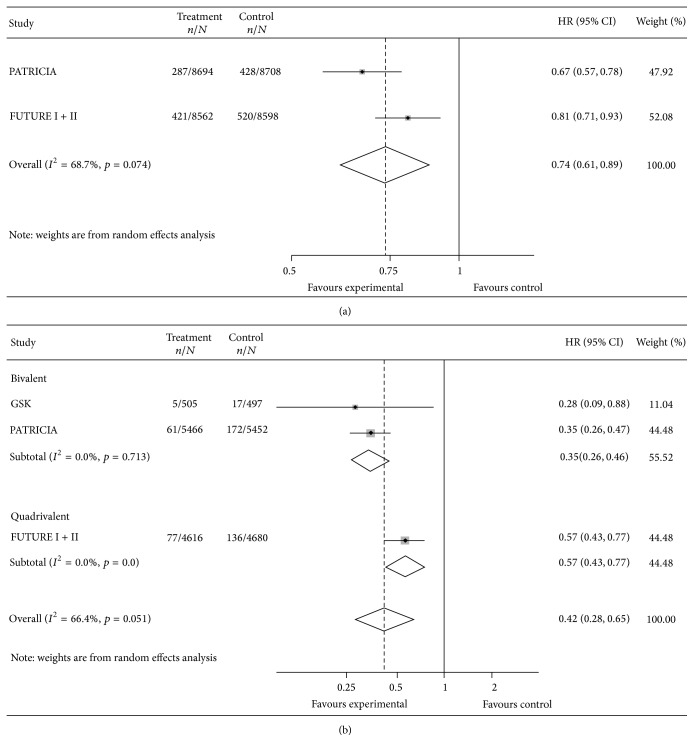
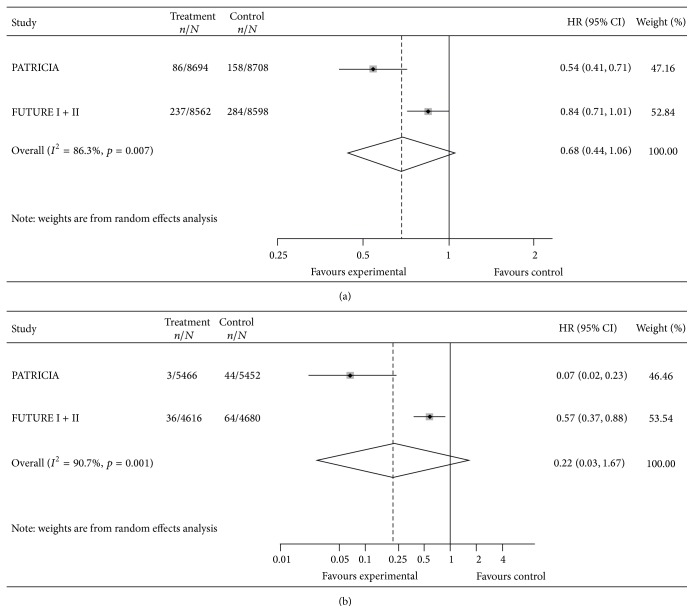
Results: Nine reports (38,419 women) were included. At enrollment mean age of women was 20 years, 90% had negative cytology, and 80% were seronegative and/or DNA negative for HPV 16 or 18 (naïve women). In the TVC-naïve, VE against CIN2+ was 58% (95% CI: 35, 72); heterogeneity was detected, VE being 65% (95% CI: 54, 74) for the bivalent and 43% (95% CI: 23, 57) for the quadrivalent. VE against CIN3+ was 78% (95% CI: <0, 97); heterogeneity was substantial, VE being 93% (95% CI: 77, 98) for the bivalent and 43% (95% CI: 12, 63) for the quadrivalent. VE in the TVC was much lower. No sufficient data were available on AIS.
Conclusions: In naïve girls bivalent vaccine shows higher efficacy, even if the number of events detected is low. In women already infected the benefit of the vaccination seems negligible.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
