

Trends in Expanded-Spectrum Cephalosporin-Resistant Escherichia coli and Klebsiella pneumoniae among Dutch Clinical Isolates, from 2008 to 2012
- PMID: 26381746
- PMCID: PMC4575062
- DOI: 10.1371/journal.pone.0138088
Trends in Expanded-Spectrum Cephalosporin-Resistant Escherichia coli and Klebsiella pneumoniae among Dutch Clinical Isolates, from 2008 to 2012
Abstract
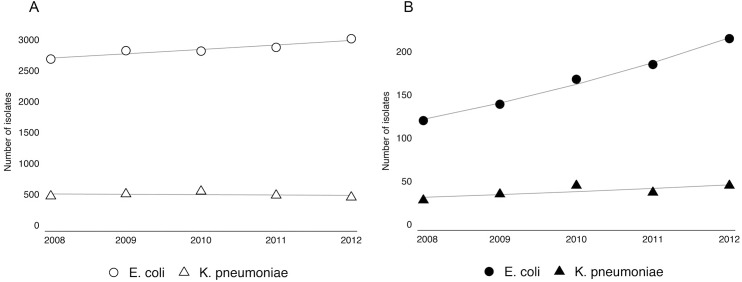
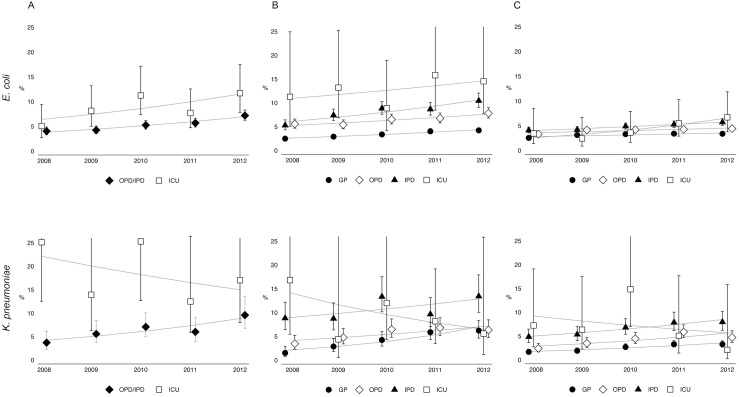
We investigated time trends in extended-spectrum cephalosporin-resistant Escherichia coli and Klebsiella pneumoniae isolates from different patient settings in The Netherlands from 2008-2012. E. coli and K. pneumoniae isolates from blood and urine samples of patients > = 18 years were selected from the Dutch Infectious Disease Surveillance System-Antimicrobial Resistance (ISIS-AR) database. We used multivariable Poisson regression to study the rate per year of blood stream infections by susceptible and resistant isolates, and generalized estimating equation (GEE) log-binomial regression for trends in the proportion of extended-spectrum cephalosporin-resistant isolates. Susceptibility data of 197,513 E. coli and 38,244 K. pneumoniae isolates were included. The proportion of extended-spectrum cephalosporin-resistant E. coli and K. pneumoniae isolates from urine and blood samples increased in all patient settings, except for K. pneumoniae isolates from patients admitted to intensive care units. For K. pneumoniae, there was a different time trend between various patient groups (p<0.01), with a significantly higher increase in extended-spectrum cephalosporin-resistant isolates from patients attending a general practitioner than in isolates from hospitalized patients. For E. coli, the increasing time trends did not differ among different patient groups. This nationwide study shows a general increase in extended-spectrum cephalosporin-resistant E. coli and K. pneumoniae isolates. However, differences in trends between E. coli en K. pneumoniae underline the importance of E. coli as a community-pathogen and its subsequent influence on hospital resistance level, while for K. pneumoniae the level of resistance within the hospital seems less influenced by the resistance trends in the community.
Conflict of interest statement
Figures

References
-
- Lee SY, Kotapati S, Kuti JL, Nightingale CH, Nicolau DP. (2006) Impact of extended-spectrum b-lactamase–producing Escherichia coli and Klebsiella species on clinical outcomes and hospital costs: a matched cohort study. Infect Control Hosp Epidemiol 27: 1226–1232. - PubMed
-
- Kang CI, Kim SH, Park WB, Lee KD, Kim HB, KIM EC, et al. (2004) Bloodstream infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae: risk factors for mortality and treatment outcome, with special emphasis on antimicrobial therapy. Antimicrob Agents Chemother 38: 4574–4581. - PMC - PubMed
-
- Livermore DM, Canton R, Gniadkowski M, Nordmann P, Rossolini GM, Arlet G, et al. (2007) CTX-M: changing the face of ESBLs in Europe. J Antimicrob Chemother 59: 165–174. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
