

Preoperative biliary drainage in perihilar cholangiocarcinoma: identifying patients who require percutaneous drainage after failed endoscopic drainage
- PMID: 26382308
- PMCID: PMC4745253
- DOI: 10.1055/s-0034-1392559
Preoperative biliary drainage in perihilar cholangiocarcinoma: identifying patients who require percutaneous drainage after failed endoscopic drainage
Abstract
Background and study aims: Preoperative biliary drainage is often initiated with endoscopic retrograde cholangiopancreatography (ERCP) in patients with potentially resectable perihilar cholangiocarcinoma (PHC), but additional percutaneous transhepatic catheter (PTC) drainage is frequently required. This study aimed to develop and validate a prediction model to identify patients with a high risk of inadequate ERCP drainage.
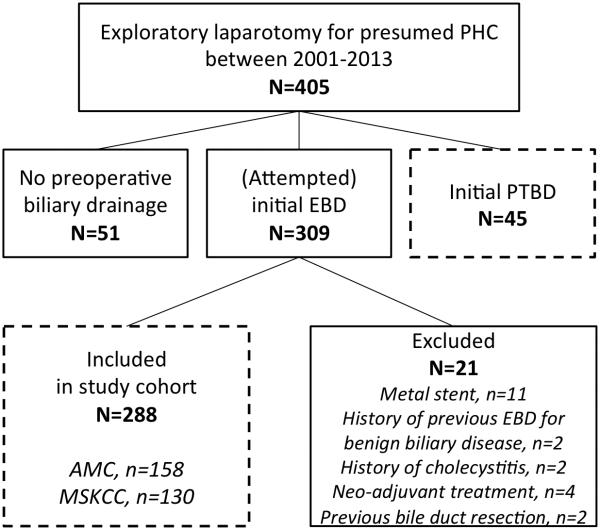
Patients and methods: Patients with potentially resectable PHC and (attempted) preoperative ERCP drainage were included from two specialty center cohorts between 2001 and 2013. Indications for additional PTC drainage were failure to place an endoscopic stent, failure to relieve jaundice, cholangitis, or insufficient drainage of the future liver remnant. A prediction model was derived from the European cohort and externally validated in the USA cohort.
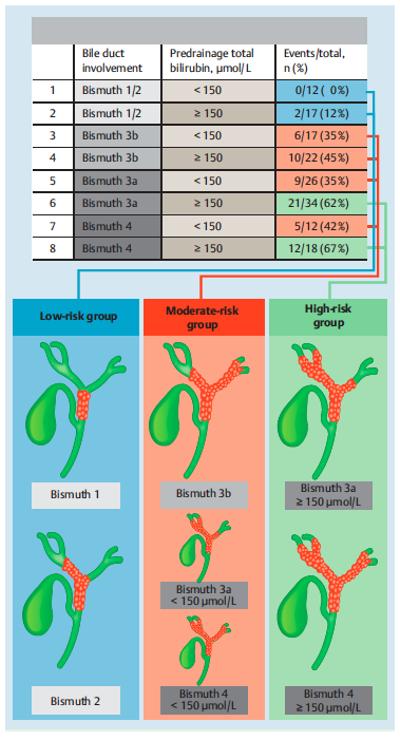
Results: Of the 288 patients, 108 (38%) required additional preoperative PTC drainage after inadequate ERCP drainage. Independent risk factors for additional PTC drainage were proximal biliary obstruction on preoperative imaging (Bismuth 3 or 4) and predrainage total bilirubin level. The prediction model identified three subgroups: patients with low risk (7%), moderate risk (40%), and high risk (62%). The high-risk group consisted of patients with a total bilirubin level above 150 µmol/L and Bismuth 3a or 4 tumors, who typically require preoperative drainage of the angulated left bile ducts. The prediction model had good discrimination (area under the curve 0.74) and adequate calibration in the external validation cohort.
Conclusions: Selected patients with potentially resectable PHC have a high risk (62%) of inadequate preoperative ERCP drainage requiring additional PTC drainage. These patients might do better with initial PTC drainage instead of ERCP.
© Georg Thieme Verlag KG Stuttgart · New York.
Figures
Comment in
-
Commentaire du travail de Wiggers JK et al., pp. 1124.Endoscopy. 2015 Dec;47(12):1197. Endoscopy. 2015. PMID: 26966737 French. No abstract available.
Similar articles
-
A Comparison of Preoperative Biliary Drainage Methods for Perihilar Cholangiocarcinoma: Endoscopic versus Percutaneous Transhepatic Biliary Drainage.Gut Liver. 2015 Nov 23;9(6):791-9. doi: 10.5009/gnl14243. Gut Liver. 2015. PMID: 26087784 Free PMC article.
-
Preoperative endoscopic versus percutaneous transhepatic biliary drainage in potentially resectable perihilar cholangiocarcinoma (DRAINAGE trial): design and rationale of a randomized controlled trial.BMC Gastroenterol. 2015 Feb 14;15:20. doi: 10.1186/s12876-015-0251-0. BMC Gastroenterol. 2015. PMID: 25887103 Free PMC article. Clinical Trial.
-
Comparing the efficacy of initial percutaneous transhepatic biliary drainage and endoscopic retrograde cholangiopancreatography with stenting for relief of biliary obstruction in unresectable cholangiocarcinoma.Surg Endosc. 2020 Mar;34(3):1186-1190. doi: 10.1007/s00464-019-06871-2. Epub 2019 May 28. Surg Endosc. 2020. PMID: 31139984
-
Preoperative Biliary Drainage in Patients with Resectable Perihilar Cholangiocarcinoma: Is Percutaneous Transhepatic Biliary Drainage Safer and More Effective than Endoscopic Biliary Drainage? A Meta-Analysis.J Vasc Interv Radiol. 2017 Apr;28(4):576-582. doi: 10.1016/j.jvir.2016.12.1218. J Vasc Interv Radiol. 2017. PMID: 28343588 Review.
-
Endoscopic ultrasound-guided biliary drainage of hilar biliary obstruction.J Hepatobiliary Pancreat Sci. 2015 Sep;22(9):664-8. doi: 10.1002/jhbp.271. Epub 2015 Jul 15. J Hepatobiliary Pancreat Sci. 2015. PMID: 26178753 Review.
Cited by
-
External biliary drainage following major liver resection for perihilar cholangiocarcinoma: impact on development of liver failure and biliary leakage.HPB (Oxford). 2016 Apr;18(4):348-53. doi: 10.1016/j.hpb.2015.11.007. Epub 2016 Feb 18. HPB (Oxford). 2016. PMID: 27037204 Free PMC article.
-
Malignant Biliary Obstruction: Evidence for Best Practice.Gastroenterol Res Pract. 2016;2016:3296801. doi: 10.1155/2016/3296801. Epub 2016 Feb 11. Gastroenterol Res Pract. 2016. PMID: 26981114 Free PMC article. Review.
-
Ablation with irreversible electroporation in patients with advanced perihilar cholangiocarcinoma (ALPACA): a multicentre phase I/II feasibility study protocol.BMJ Open. 2017 Sep 1;7(9):e015810. doi: 10.1136/bmjopen-2016-015810. BMJ Open. 2017. PMID: 28864693 Free PMC article. Clinical Trial.
-
Postbiliary drainage rates of cholangitis are impacted by procedural technique for patients with supra-ampullary cholangiocarcinoma: A SEER-Medicare analysis.J Surg Oncol. 2019 Aug;120(2):249-255. doi: 10.1002/jso.25485. Epub 2019 May 1. J Surg Oncol. 2019. PMID: 31044430 Free PMC article.
-
Feasibility of EUS-guided hepaticogastrostomy for inoperable malignant hilar biliary strictures.Endosc Ultrasound. 2021 Jan-Feb;10(1):51-56. doi: 10.4103/eus.eus_68_20. Endosc Ultrasound. 2021. PMID: 33402550 Free PMC article.
References
-
- Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362:1273–1281. - PubMed
-
- Ebata T, Kosuge T, Hirano S, et al. Proposal to modify the International Union Against Cancer staging system for perihilar cholangiocarcinomas. Br J Surg. 2014;101:79–88. - PubMed
-
- Matsuo K, Rocha FG, Ito K, et al. The Blumgart preoperative staging system for hilar cholangiocarcinoma: analysis of resectability and outcomes in 380 patients. J Am Coll Surg. 2012;215:343–355. - PubMed
-
- Nuzzo G, Giuliante F, Ardito F, et al. Improvement in perioperative and long-term outcome after surgical treatment of hilar cholangiocarcinoma: results of an Italian multicenter analysis of 440 patients. Arch Surg. 2012;147:26–34. - PubMed
-
- Nagino M, Ebata T, Yokoyama Y, et al. Evolution of surgical treatment for perihilar cholangiocarcinoma: a single-center 34-year review of 574 consecutive resections. Ann Surg. 2013;258:129–140. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
