

Missed Opportunities for TB Investigation in Primary Care Clinics in South Africa: Experience from the XTEND Trial
- PMID: 26383102
- PMCID: PMC4575203
- DOI: 10.1371/journal.pone.0138149
Missed Opportunities for TB Investigation in Primary Care Clinics in South Africa: Experience from the XTEND Trial
Abstract
Setting: 40 primary health clinics (PHCs) in four provinces in South Africa, June 2012 -February 2013.
Objective: To determine whether health care worker (HCW) practice in investigating people with TB symptoms was altered when the initial test for TB was changed from smear microscopy to Xpert MTB/RIF.
Design: Cross-sectional substudy at clinics participating in a pragmatic cluster randomised trial, Xpert for TB: Evaluating a New Diagnostic "XTEND", which evaluated the effect of Xpert MTB/RIF implementation in South Africa.
Methods: Consecutive adults exiting PHCs reporting at least one TB symptom (defined as any of cough, weight loss, night sweats and fever) were enrolled. The main outcome was the proportion who self-reported having sputum requested by HCW during the clinic encounter just completed.
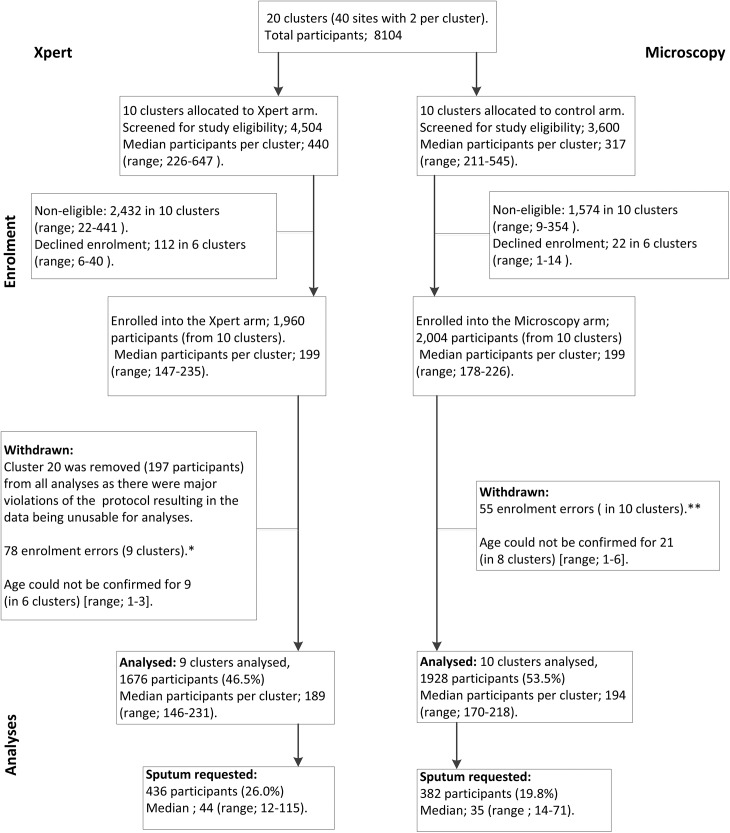
Results: 3604 adults exiting PHCs (1676 in Xpert arm, 1928 in microscopy arm) were enrolled (median age 38 years, 71.4% female, 38.8% reported being HIV-positive, 70% reported cough). For 1267 participants (35.2%) the main reason for attending the clinic was TB symptom(s). Overall 2130/3604 (59.1%) said they reported their symptom(s) to HCW. 22.7% (818/3604) reported having been asked to give sputum for TB investigation. Though participants in the Xpert vs. microscopy arm were more likely to have sputum requested by HCW, this was not significantly different: overall (26.0% [436/1676] vs 19.8% [382/1928]; adjusted prevalence ratio [aPR] 1.31, [95% CI 0.78-2.20]) and when restricted to those presenting at clinics due to symptoms (49.1% [260/530] vs 29.9% [220/737]; aPR 1.38 [0.89-2.13]) and those reporting being HIV-positive (29.4% [190/647] vs 20.8% [156/749]; aPR 1.38[0.88-2.16]). Those attending clinic due to TB symptoms, were more likely to have sputum requested if they had increasing number of symptoms; longer duration of cough, unintentional weight loss and night sweats and if they reported symptoms to HCW.
Conclusions: A large proportion of people exiting PHCs reporting TB symptoms did not get tested. Implementation of Xpert MTB/RIF did not substantially change the probability of testing for TB. Better systems are needed to ensure that opportunities to identify active TB among PHC attendees are not missed.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Global Tuberculosis report 2013. Available: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf. Accessed 3 October 2014.
-
- Getahun H, Harrington M, O'Brien R, Nunn P. Diagnosis of smear-negative pulmonary tuberculosis in people with HIV infection of AIDS in resource-constrained settings: informing urget policy changes. Lancet 2007; 369: 2042–9. - PubMed
-
- World Health Organization. Guidelines on intensified tuberculosis case finding and isoniazid preventive therapy for people living with HIV in resource constrained setting Geneva, Switzerland: WHO, 2011. Available: http://whqlibdoc.who.int/publications/2011/9789241500708_eng.pdf. Accessed 6 January 2015.
-
- WHO Three I’s Meeting: Intensified Case-Finding (ICF), Isoniazid Preventive Therapy (IPT) and TB Infection Control (IC) for People Living with HIV. Report of a Joint WHO HIV/AIS and TB Department Meeting. 2–4 April 2008, Geneva, Switzerland. Available www.who.int/hiv/pub/meetingreports/WHO_3Is_meeting_report.pdf?ua=1. Accessed 7 January 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
