

Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms
- PMID: 26383759
- PMCID: PMC4602246
- DOI: 10.1136/bjsports-2015-h2747rep
Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms
Abstract
Objective: To determine benefits and harms of arthroscopic knee surgery involving partial meniscectomy, debridement, or both for middle aged or older patients with knee pain and degenerative knee disease.
Design: Systematic review and meta-analysis.
Main outcome measures: Pain and physical function.
Data sources: Systematic searches for benefits and harms were carried out in Medline, Embase, CINAHL, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL) up to August 2014. Only studies published in 2000 or later were included for harms.
Eligibility criteria for selecting studies: Randomised controlled trials assessing benefit of arthroscopic surgery involving partial meniscectomy, debridement, or both for patients with or without radiographic signs of osteoarthritis were included. For harms, cohort studies, register based studies, and case series were also allowed.
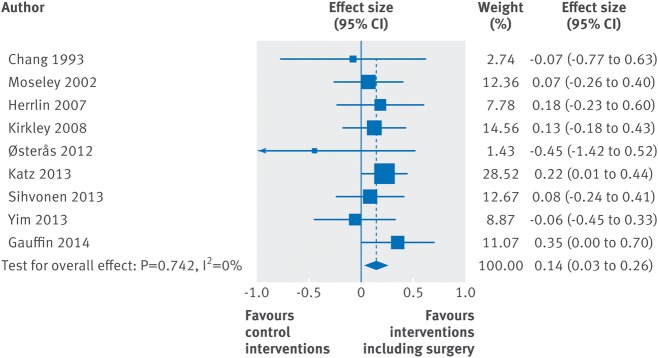
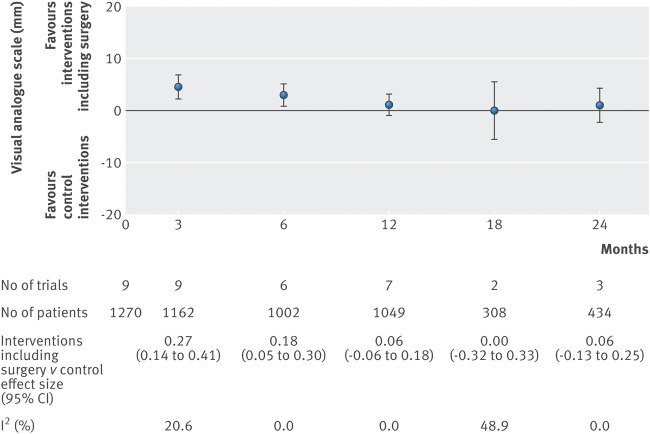
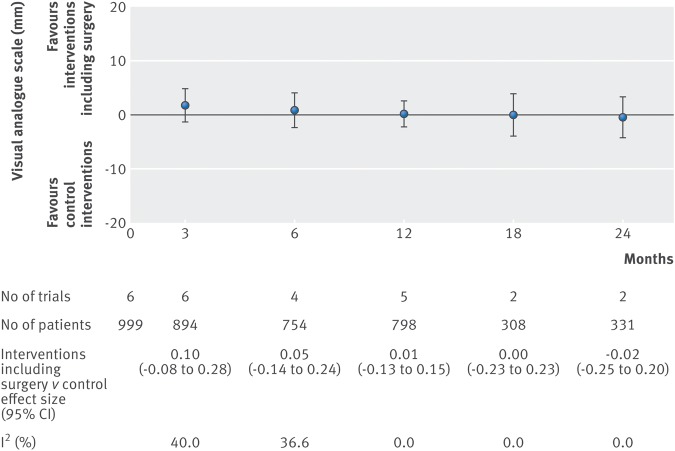
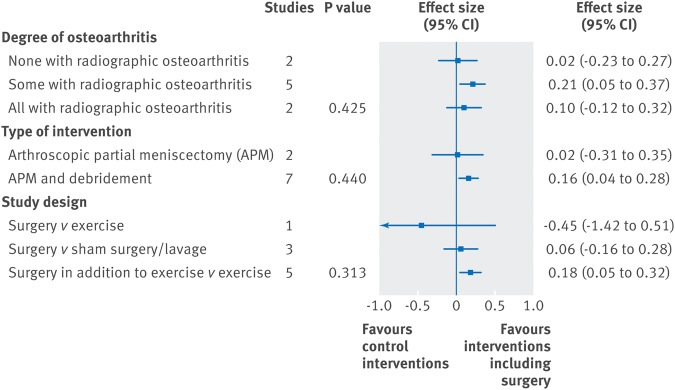
Results: The search identified nine trials assessing the benefits of knee arthroscopic surgery in middle aged and older patients with knee pain and degenerative knee disease. The main analysis, combining the primary endpoints of the individual trials from three to 24 months postoperatively, showed a small difference in favour of interventions including arthroscopic surgery compared with control treatments for pain (effect size 0.14, 95% confidence interval 0.03 to 0.26). This difference corresponds to a benefit of 2.4 (95% confidence interval 0.4 to 4.3) mm on a 0-100 mm visual analogue scale. When analysed over time of follow-up, interventions including arthroscopy showed a small benefit of 3-5 mm for pain at three and six months but not later up to 24 months. No significant benefit on physical function was found (effect size 0.09, -0.05 to 0.24). Nine studies reporting on harms were identified. Harms included symptomatic deep venous thrombosis (4.13 (95% confidence interval 1.78 to 9.60) events per 1000 procedures), pulmonary embolism, infection, and death.
Conclusions: The small inconsequential benefit seen from interventions that include arthroscopy for the degenerative knee is limited in time and absent at one to two years after surgery. Knee arthroscopy is associated with harms. Taken together, these findings do not support the practise of arthroscopic surgery for middle aged or older patients with knee pain with or without signs of osteoarthritis.
Systematic review registration: PROSPERO CRD42014009145.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

Republished from
-
Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms.BMJ. 2015 Jun 16;350:h2747. doi: 10.1136/bmj.h2747. BMJ. 2015. PMID: 26080045 Free PMC article.
References
-
- Hawker G, Guan J, Judge A, et al. . Knee arthroscopy in England and Ontario: patterns of use, changes over time, and relationship to total knee replacement. J Bone Joint Surg Am 2008;90:2337–45. - PubMed
-
- Cullen K, Hall M, Golosinskiya A. Ambulatory surgery in the United States, 2006. National Center for Health Statistics, 2009. - PubMed
-
- Lazic S, Boughton O, Hing C, et al. . Arthroscopic washout of the knee: a procedure in decline. Knee 2014;21:631–4. - PubMed
-
- Englund M, Niu J, Guermazi A, et al. . Effect of meniscal damage on the development of frequent knee pain, aching, or stiffness. Arthritis Rheum 2007;56:4048–54. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases