

Local Oestrogen for Pelvic Floor Disorders: A Systematic Review
- PMID: 26383760
- PMCID: PMC4575150
- DOI: 10.1371/journal.pone.0136265
Local Oestrogen for Pelvic Floor Disorders: A Systematic Review
Abstract
Objective: The decline in available oestrogen after menopause is a possible etiological factor in pelvic floor disorders like vaginal atrophy (VA), urinary incontinence (UI), overactive bladder (OAB) and pelvic organ prolapse (POP). This systematic review will examine the evidence for local oestrogen therapy in the treatment of these pelvic floor disorders.
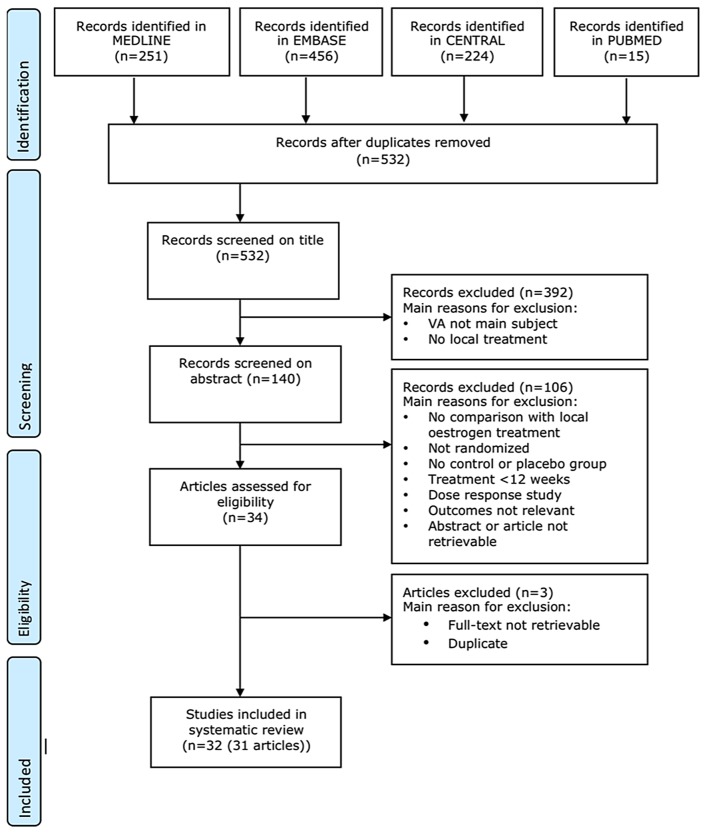
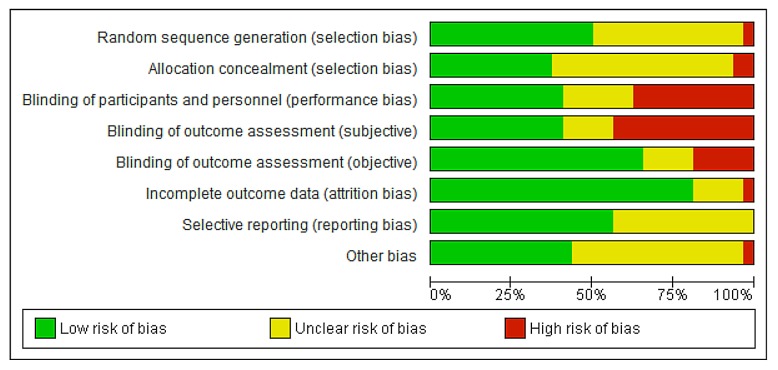
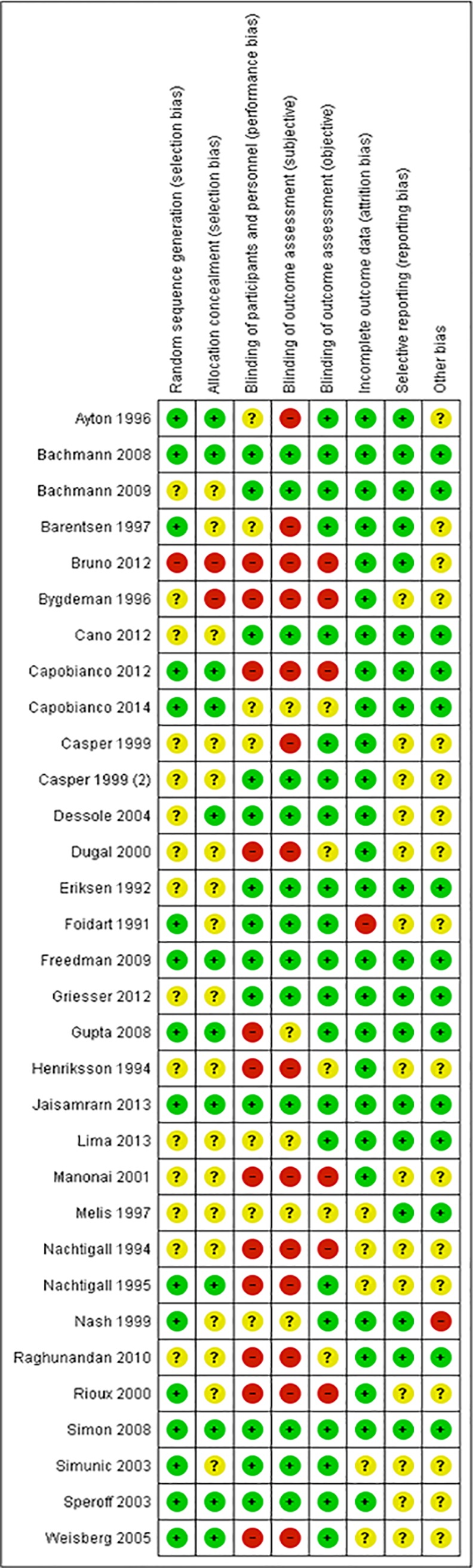
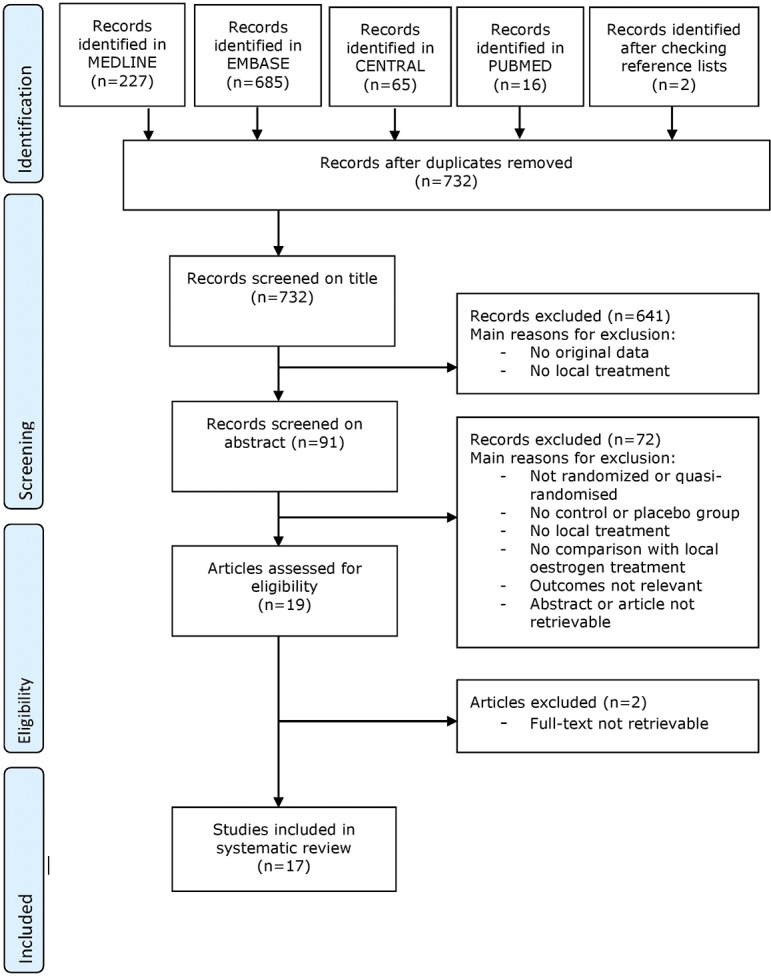
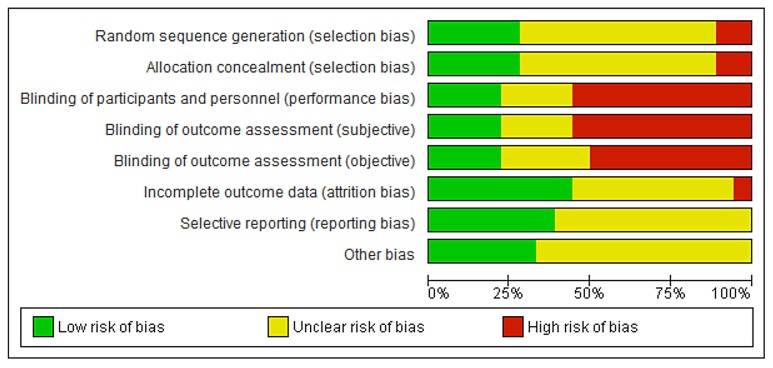
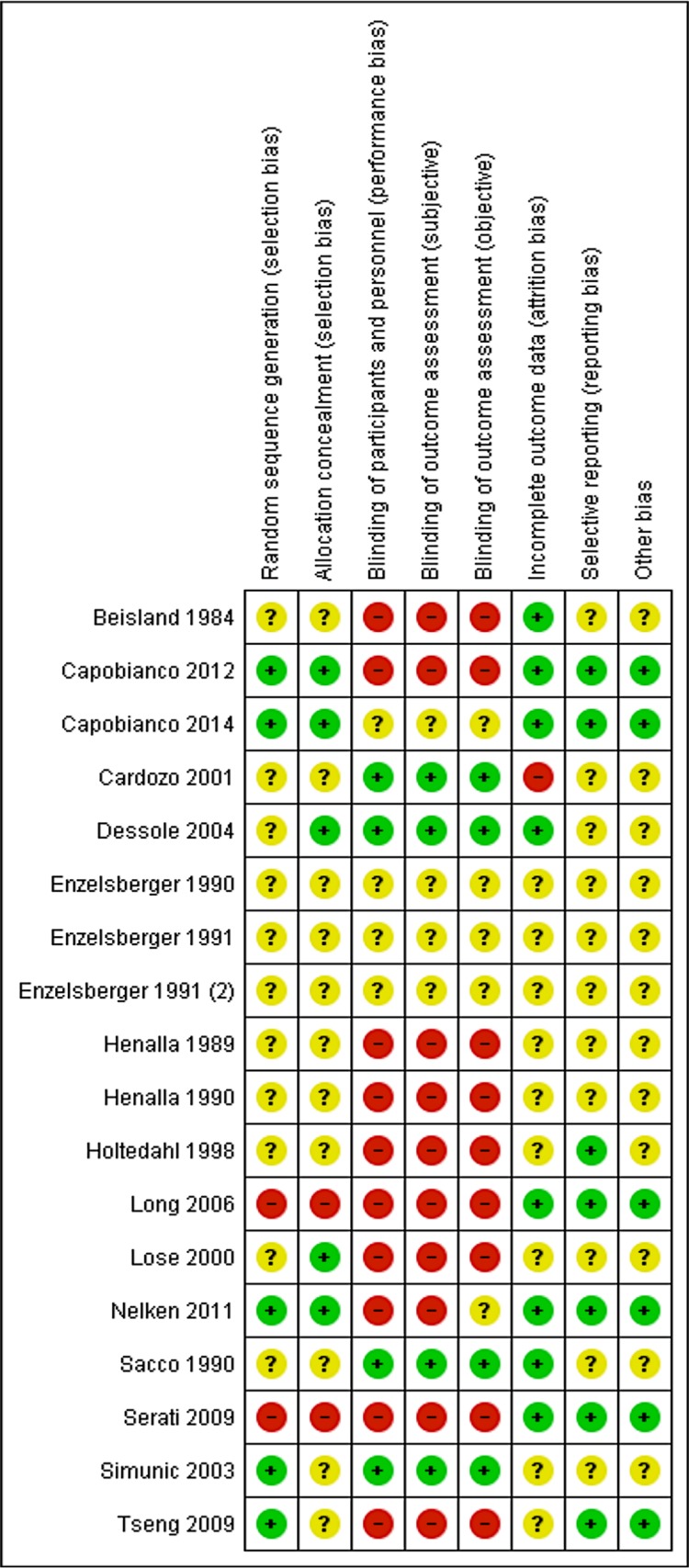
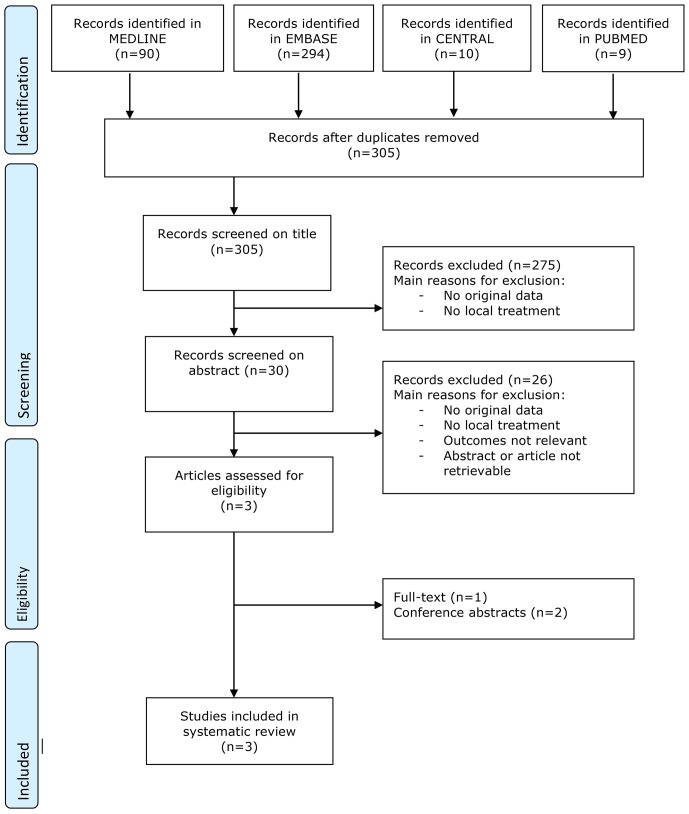
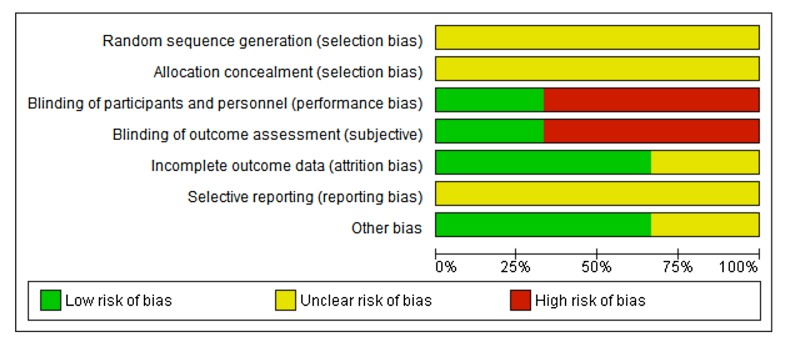
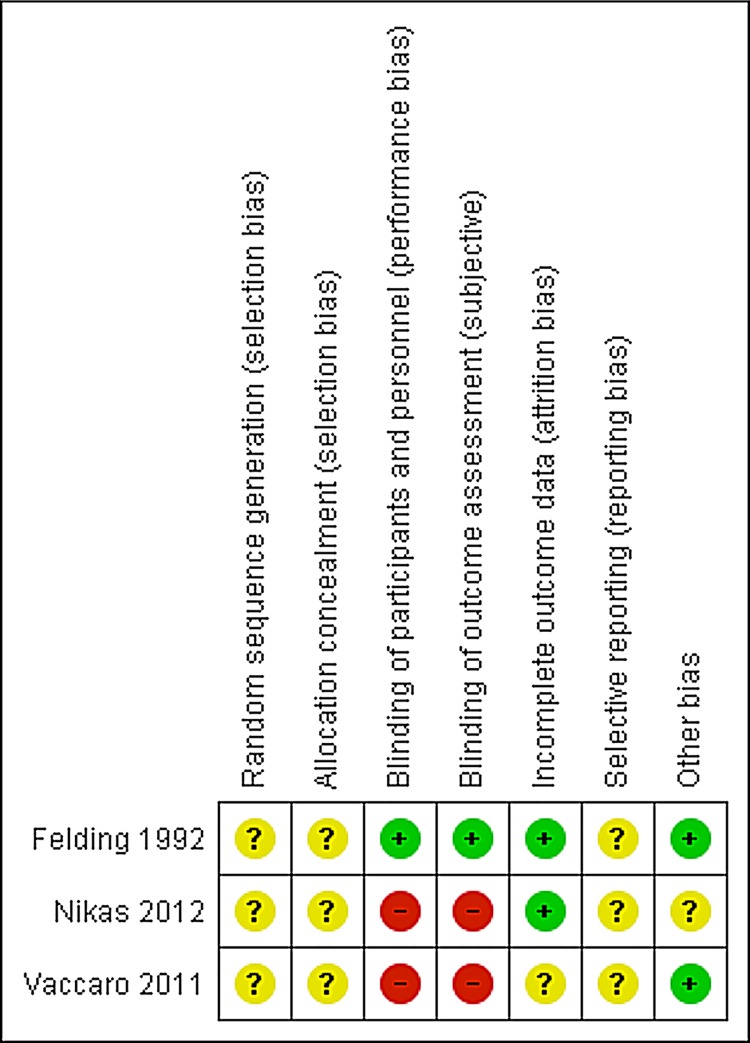
Evidence acquisition: We performed a systematic search in MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials and the non-MEDLINE subset of PubMed from inception to May 2014. We searched for local oestrogens and VA (I), UI/OAB (II) and POP (III). Part I was combined with broad methodological filters for randomized controlled trials (RCTs) and secondary evidence. For part I and II two reviewers independently selected RCTs evaluating the effect of topical oestrogens on symptoms and signs of VA and UI/OAB. In part III all studies of topical oestrogen therapy in the treatment of POP were selected. Data extraction and the assessment of risk of bias using the Cochrane Risk of Bias Tool was undertaken independently by two reviewers.
Evidence synthesis: The included studies varied in ways of topical application, types of oestrogen, dosage and treatment durations. Objective and subjective outcomes were assessed by a variety of measures. Overall, subjective and urodynamic outcomes, vaginal maturation and vaginal pH changed in favor of vaginal oestrogens compared to placebo. No obvious differences between different application methods were revealed. Low doses already seemed to have a beneficial effect. Studies evaluating the effect of topical oestrogen in women with POP are scarce and mainly assessed symptoms and signs associated with VA instead of POP symptoms.
Conclusion: Topical oestrogen administration is effective for the treatment of VA and seems to decrease complaints of OAB and UI. The potential for local oestrogens in the prevention as well as treatment of POP needs further research.
Conflict of interest statement
Figures
References
-
- Iosif CS, Batra S, Ek A, Astedt B (1981) Estrogen receptors in the human female lower uninary tract. AmJObstetGynecol 141: 817–820. - PubMed
-
- Chung dJ, Bai SW (2006) Roles of sex steroid receptors and cell cycle regulation in pathogenesis of pelvic organ prolapse. CurrOpinObstetGynecol 18: 551–554. - PubMed
-
- Rud T, Andersson KE, Asmussen M, Hunting A, Ulmsten U (1980) Factors maintaining the intraurethral pressure in women. Invest Urol 17: 343–347. - PubMed
-
- Matsubara S, Okada H, Shirakawa T, Gotoh A, Kuno T, et al. (2002) Estrogen levels influence beta-3-adrenoceptor-mediated relaxation of the female rat detrusor muscle. Urology 59: 621–625. - PubMed
-
- Shenfeld OZ, McCammon KA, Blackmore PF, Ratz PH (1999) Rapid effects of estrogen and progesterone on tone and spontaneous rhythmic contractions of the rabbit bladder. Urol Res 27: 386–392. - PubMed
