

Rates of Retinal Nerve Fiber Layer Loss in Contralateral Eyes of Glaucoma Patients with Unilateral Progression by Conventional Methods
- PMID: 26383993
- PMCID: PMC4624038
- DOI: 10.1016/j.ophtha.2015.07.027
Rates of Retinal Nerve Fiber Layer Loss in Contralateral Eyes of Glaucoma Patients with Unilateral Progression by Conventional Methods
Abstract
Purpose: To determine whether progressive retinal nerve fiber layer (RNFL) loss occurs in the contralateral eye of patients with glaucoma showing unilateral progression according to conventional diagnostic methods.
Design: Prospective, longitudinal, observational cohort study.
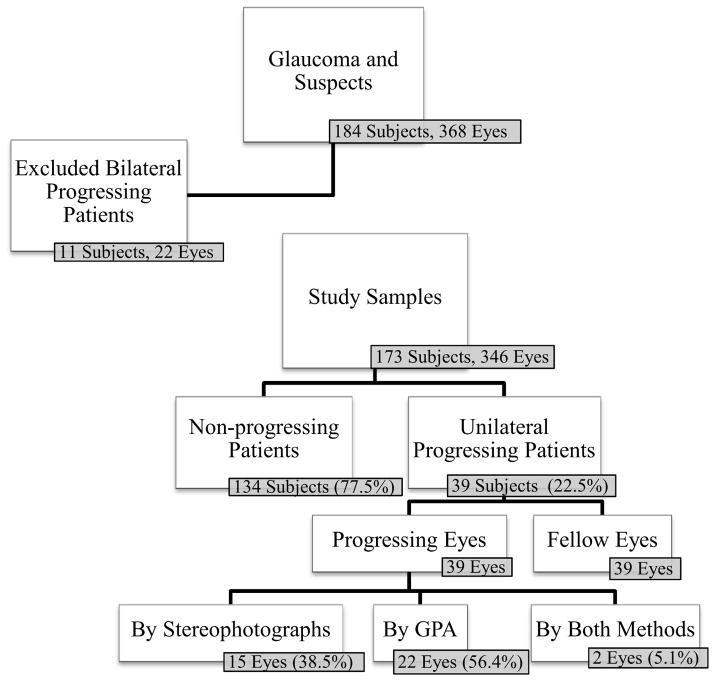
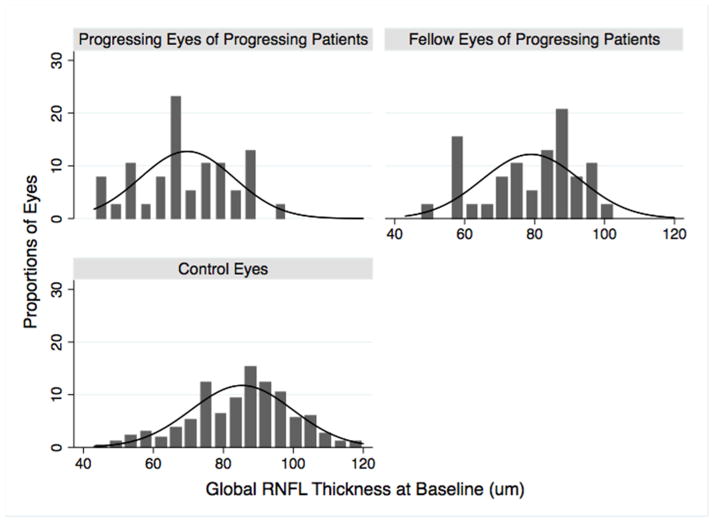
Participants: Three hundred forty-six eyes of 173 patients (118 eyes with glaucoma and 228 eyes with suspect glaucoma at baseline) followed up for an average of 3.5±0.7 years.
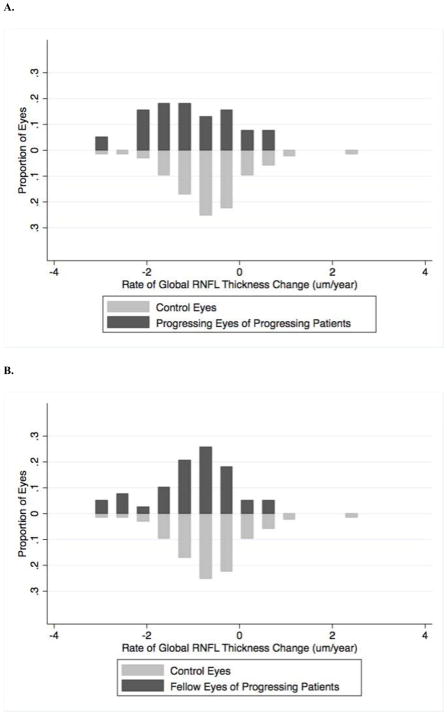
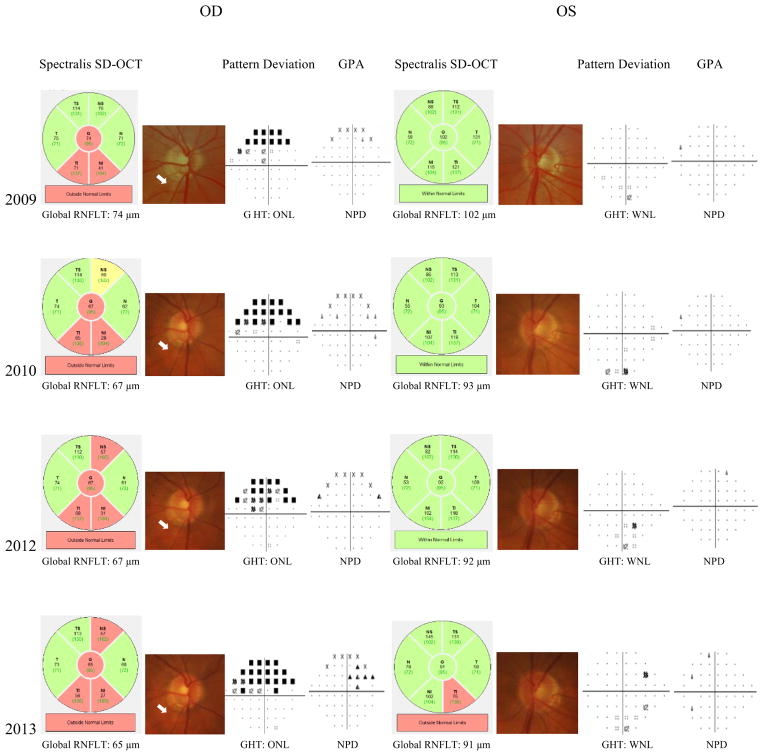
Methods: All subjects underwent standard automated perimetry (SAP; Humphrey Field Analyzer; Carl Zeiss Meditec, Dublin, CA) and spectral-domain (SD) optical coherence tomography (OCT; Spectralis; Heidelberg Engineering, Inc., Carlsbad, CA) in both eyes at 6-month intervals. Eyes were determined as progressing by conventional methods if there was progression on masked grading of optic disc stereophotographs or SAP Guided Progression Analysis (GPA; Carl Zeiss Meditec; "likely progression"). Rates of change in SD OCT average RNFL thickness were obtained using a linear mixed effects model. Rate of global loss was calculated using a random coefficient model and compared for nonprogressing patients, progressing eyes, and fellow eyes of unilateral progressing patients.
Main outcomes measures: Rate of change in global RNFL thickness.
Results: Thirty-nine subjects showed evidence of unilateral progression by GPA, disc photographs, or both during follow-up. Mean ± standard error rate of RNFL loss in eyes progressing by conventional methods was -0.89±0.22 μm/year (P<0.001). The contralateral eyes of these subjects also showed significant loss of RNFL over time (-1.00±0.20 μm/year; P<0.001). One hundred thirty-four subjects did not show progression by conventional methods in either eye. These eyes also showed a significant decline over time in average RNFL thickness (-0.71±0.09 μm/year; P<0.001); however, the rate of change in these eyes was slower than that of the contralateral eye of patients showing unilateral progression (P<0.001).
Conclusions: Loss of RNFL thickness was seen in a substantial number of contralateral eyes of glaucoma patients showing unilateral progression by conventional methods. These findings indicate that assessment of RNFL thickness by SD OCT may show progressive glaucomatous damage that is not detected by visual fields or optic disc stereophotography.
Copyright © 2015 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
T.L. – none; A.J.T. – research support from Heidelberg Engineering; C.P.B.G. – none; L.M.Z. - research support from National Eye Institute, Carl Zeiss Meditec, Heidelberg Engineering, Optovue, Topcon; R.N.W. – research support from Carl Zeiss Meditec, Genentech, Heidelberg Engineering, Nidek, Novartis, Optovue, Topcon; Consultant for Alcon, Allergan, Bausch & Lomb, Carl Zeiss Meditec, Topcon; F.A.M. – research support from Alcon Laboratories, Allergan, Bausch & Lomb, Carl Zeiss Meditec, Heidelberg Engineering, Merck, Reichert, Sensimed, Topcon, National Eye Institute; Consultant for Alcon, Allergan, Reichert.
Figures
References
-
- Artes PH, O’leary N, Nicolela MT, et al. Visual field progression in glaucoma: what is the specificity of the guided progression analysis? Ophthalmology. 2014;121:2023–7. - PubMed
-
- Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
