

Trends and interaction of polypharmacy and potentially inappropriate prescribing in primary care over 15 years in Ireland: a repeated cross-sectional study
- PMID: 26384726
- PMCID: PMC4577876
- DOI: 10.1136/bmjopen-2015-008656
Trends and interaction of polypharmacy and potentially inappropriate prescribing in primary care over 15 years in Ireland: a repeated cross-sectional study
Abstract
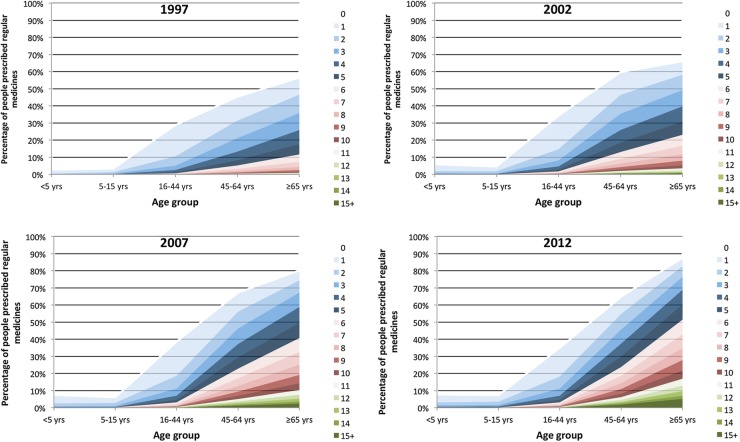
Objectives: To examine: (1) changes in polypharmacy in 1997, 2002, 2007 and 2012 and; (2) changes in potentially inappropriate prescribing (PIP) prevalence and the relationship between PIP and polypharmacy in individuals aged ≥65 years over this period in Ireland.
Methods: This repeated cross-sectional study using pharmacy claims data included all individuals eligible for the General Medical Services scheme in the former Eastern Health Board region of Ireland in 1997, 2002, 2007 and 2012 (range 338,025-539,752 individuals). Outcomes evaluated were prevalence of polypharmacy (being prescribed ≥5 regular medicines) and excessive polypharmacy (≥10 regular medicines) in all individuals and PIP prevalence in those aged ≥65 years determined by 30 criteria from the Screening Tool for Older Persons' Prescriptions.
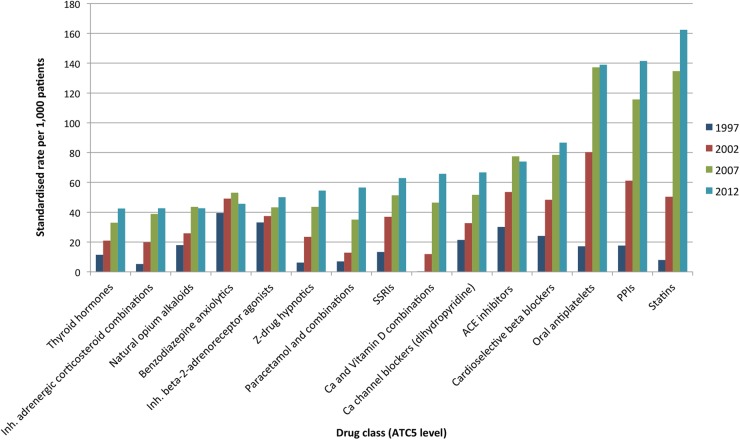
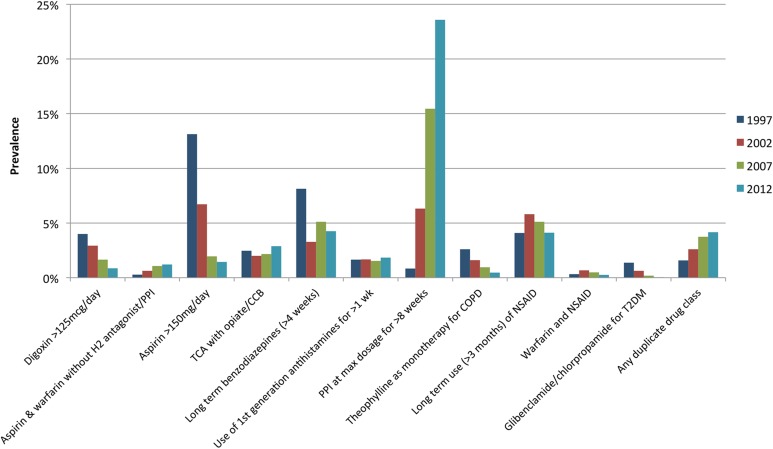
Results: The prevalence of polypharmacy increased from 1997 to 2012, particularly among older individuals (from 17.8% to 60.4% in those aged ≥65 years). The adjusted incident rate ratio for polypharmacy in 2012 compared to 1997 was 4.16 (95% CI 3.23 to 5.36), and for excessive polypharmacy it was 10.53 (8.58 to 12.91). Prevalence of PIP rose from 32.6% in 1997 to 37.3% in 2012. High-dose aspirin and digoxin prescribing decreased over time, but long-term proton pump inhibitors at maximal dose increased substantially (from 0.8% to 23.8%). The odds of having any PIP in 2012 were lower compared to 1997 after controlling for gender and level of polypharmacy, OR 0.39 (95% CI 0.39 to 0.4).
Conclusions: Accounting for the marked increase in polypharmacy, prescribing quality appears to have improved with a reduction in the odds of having PIP from 1997 to 2012. With growing numbers of people taking multiple regular medicines, strategies to address the related challenges of polypharmacy and PIP are needed.
Keywords: CLINICAL PHARMACOLOGY; EPIDEMIOLOGY; PRIMARY CARE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- IMS Institute for Healthcare Informatics. The global use of medicines: outlook through 2016. Danbury, CT: IMS Health, 2012.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources