

Predictors of relapse and treatment outcomes in biopsy-proven giant cell arteritis: a retrospective cohort study
- PMID: 26385368
- PMCID: PMC4939727
- DOI: 10.1093/rheumatology/kev348
Predictors of relapse and treatment outcomes in biopsy-proven giant cell arteritis: a retrospective cohort study
Abstract
Objective: To evaluate characteristics of relapse, relapse rates, treatment and outcomes among patients with biopsy-proven GCA in a large, single-institution cohort.
Methods: We conducted a retrospective review of all patients with biopsy-proven GCA from 1998 to 2013. Demographic, clinical, laboratory and treatment data at presentation and during follow-up were collected. Comparisons by relapse rate were performed using chi-square tests. Prednisone discontinuation by initial oral dose ≤40 and >40 mg/day was compared using Cox models.
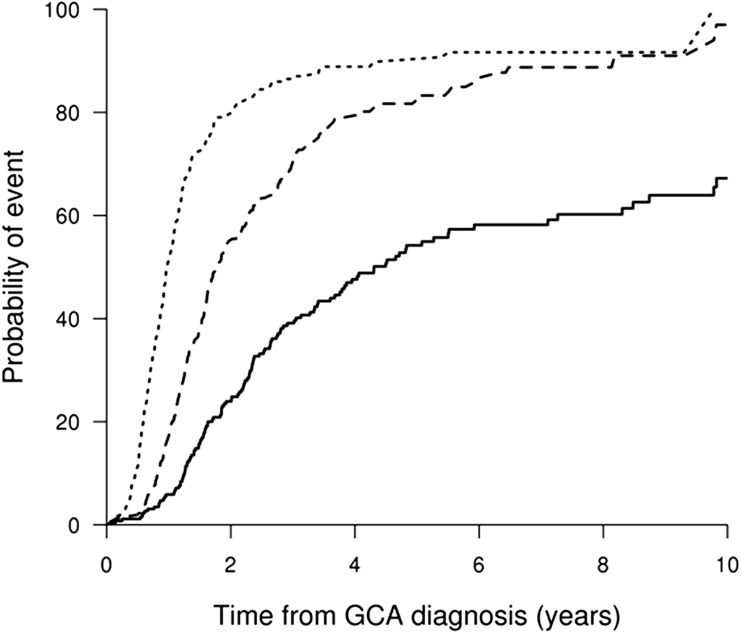
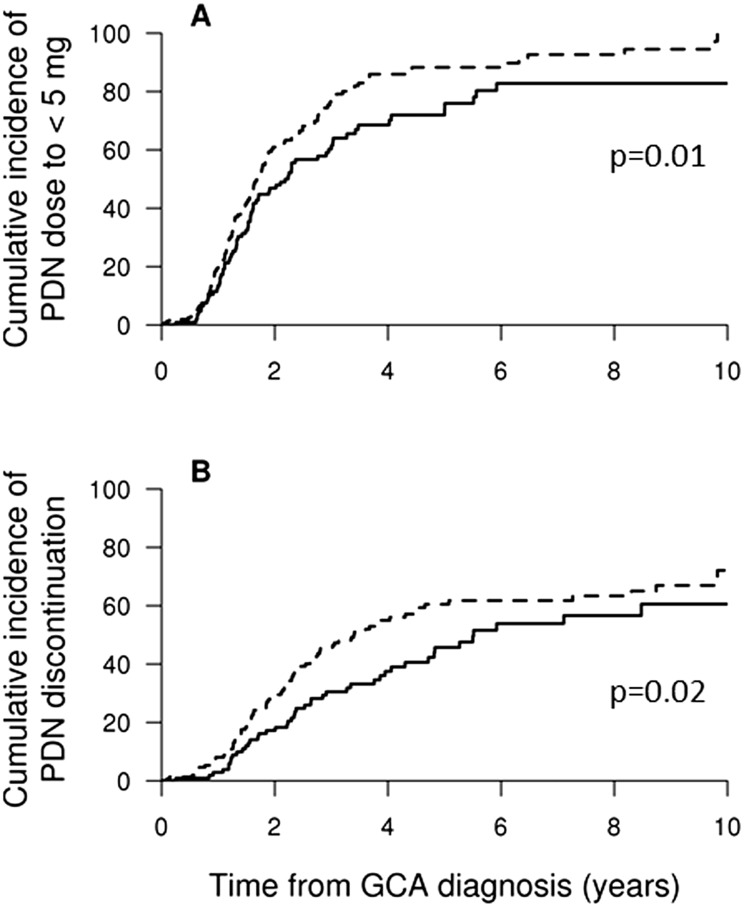
Results: The cohort included 286 patients [74% female, mean age at diagnosis 75.0 years (s.d. 7.6), median follow-up 5.1 years). During follow-up, 73 patients did not relapse, 80 patients had one relapse and 133 had two or more relapses. The first relapse occurred during the first year in 50% of patients, by 2 years in 68% and by 5 years in 79%. More patients with established hypertension (P = 0.007) and diabetes (P = 0.039) at GCA diagnosis were in the high relapse rate group ( ≥ 0.5 relapses/year) and more females were in the low or high relapse groups than in the no relapse group (P = 0.034). Patients receiving an initial oral prednisone dose >40 mg/day were able to reach a dose of <5 mg/day [hazard ratio (HR) 1.46 (95% CI 1.09, 1.96)] and discontinue prednisone [HR 1.56 (95% CI 1.09, 2.23)] sooner than patients receiving ≤40 mg/day without an increase in observed glucocorticoid-associated adverse events.
Conclusion: Females and patients with hypertension or diabetes at GCA diagnosis have more relapses during follow-up. Patients treated with an initial oral prednisone dose >40 mg/day achieved earlier prednisone discontinuation.
Keywords: adverse events; cohort; diabetes; giant cell arteritis; glucocorticoids; hypertension; relapse; retrospective.
© The Author 2015. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgia rheumatica and giant-cell arteritis. N Engl J Med 2002;347:261–71. - PubMed
-
- Baslund B, Helleberg M, Faurschou M, Obel N. Mortality in patients with giant cell arteritis. Rheumatology 2014;38:2215–7. - PubMed
-
- Matteson EL, Gold KN, Bloch DA, Hunder GG. Long-term survival of patients with giant cell arteritis in the American College of Rheumatology giant cell arteritis classification criteria cohort. Am J Med 1996;100:193–6. - PubMed
-
- Durand M, Thomas SL. Incidence of infections in patients with giant cell arteritis: a cohort study. Arthritis Care Res 2012;64:581–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
