

Prevalence, Predictors, and Outcomes of Pulmonary Hypertension in CKD
- PMID: 26386072
- PMCID: PMC4769189
- DOI: 10.1681/ASN.2014111111
Prevalence, Predictors, and Outcomes of Pulmonary Hypertension in CKD
Abstract
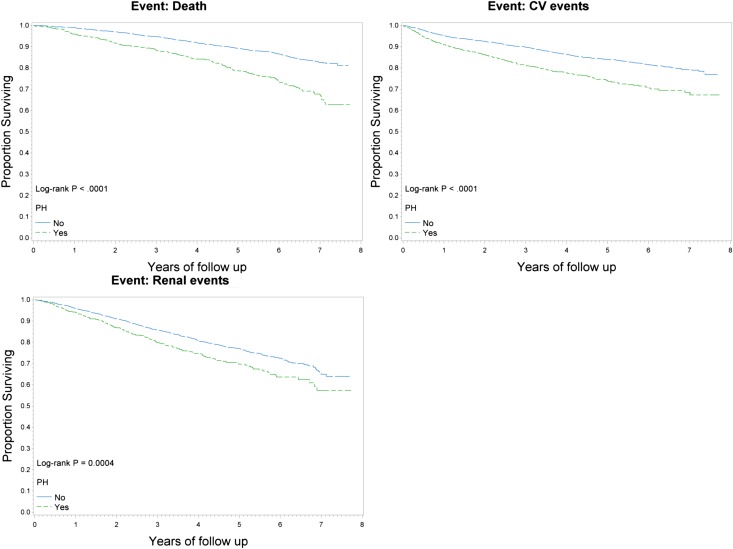
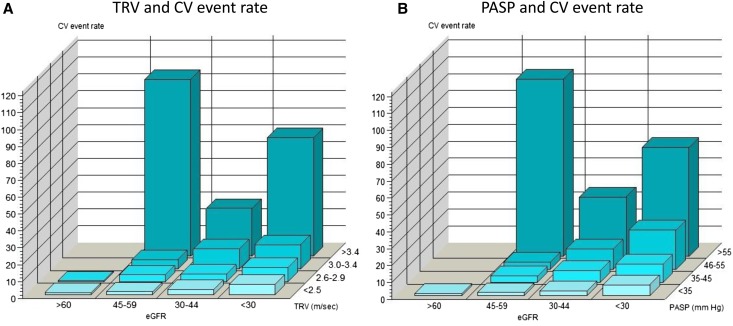
Pulmonary hypertension (PH) is associated with poor outcomes in the dialysis and general populations, but its effect in CKD is unclear. We evaluated the prevalence and predictors of PH measures and their associations with long-term clinical outcomes in patients with nondialysis-dependent CKD. Chronic Renal Insufficiency Cohort (CRIC) Study participants who had Doppler echocardiography performed were considered for inclusion. PH was defined as the presence of estimated pulmonary artery systolic pressure (PASP) >35 mmHg and/or tricuspid regurgitant velocity (TRV) >2.5 m/s. Associations between PH, PASP, and TRV and cardiovascular events, renal events, and all-cause mortality were examined using Cox proportional hazards models. Of 2959 eligible participants, 21% (n=625) had PH, with higher rates among those with lower levels of kidney function. In the multivariate model, older age, anemia, lower left ventricular ejection fraction, and presence of left ventricular hypertrophy were associated with greater odds of having PH. After adjusting for relevant confounding variables, PH was independently associated with higher risk for death (hazard ratio, 1.38; 95% confidence interval, 1.10 to 1.72) and cardiovascular events (hazard ratio, 1.23; 95% confidence interval, 1.00 to 1.52) but not renal events. Similarly, TRV and PASP were associated with death and cardiovascular events but not renal events. In this study of patients with CKD and preserved left ventricular systolic function, we report a high prevalence of PH. PH and higher TRV and PASP (echocardiographic measures of PH) are associated with adverse outcomes in CKD. Future studies may explain the mechanisms that underlie these findings.
Keywords: CKD; heart failure; mortality; pulmonary hypertension.
Copyright © 2016 by the American Society of Nephrology.
Figures
Comment in
-
Pulmonary Hypertension in CKD: Some Answers, Yet More Questions.J Am Soc Nephrol. 2016 Mar;27(3):661-3. doi: 10.1681/ASN.2015070819. Epub 2015 Sep 18. J Am Soc Nephrol. 2016. PMID: 26386071 Free PMC article. No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellström B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R, SHARP Investigators : The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo-controlled trial. Lancet 377: 2181–2192, 2011 - PMC - PubMed
-
- Jardine MJ, Kang A, Zoungas S, Navaneethan SD, Ninomiya T, Nigwekar SU, Gallagher MP, Cass A, Strippoli G, Perkovic V: The effect of folic acid based homocysteine lowering on cardiovascular events in people with kidney disease: Systematic review and meta-analysis. BMJ 344: e3533, 2012 - PMC - PubMed
-
- Norris K, Bourgoigne J, Gassman J, Hebert L, Middleton J, Phillips RA, Randall O, Rostand S, Sherer S, Toto RD, Wright JT, Jr., Wang X, Greene T, Appel LJ, Lewis J, AASK Study Group : Cardiovascular outcomes in the african american study of kidney disease and hypertension (AASK) trial. Am J Kidney Dis 48: 739–751, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- M01RR16500/RR/NCRR NIH HHS/United States
- U01-DK060980/DK/NIDDK NIH HHS/United States
- R01 DK101500/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- R01-DK101500/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- U01-DK061022/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01-DK060990/DK/NIDDK NIH HHS/United States
- U01-DK060984/DK/NIDDK NIH HHS/United States
- UL1-TR000433/TR/NCATS NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1-TR000003/TR/NCATS NIH HHS/United States
- UL1-RR029879/RR/NCRR NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1-TR000439/TR/NCATS NIH HHS/United States
- U01-DK061021/DK/NIDDK NIH HHS/United States
- UL1-RR024131/RR/NCRR NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01-DK060902/DK/NIDDK NIH HHS/United States
- U01-DK060963/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01-DK061028/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- P30-GM103337/GM/NIGMS NIH HHS/United States
- UL1-TR000424/TR/NCATS NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
