

Urine Biomarkers and Perioperative Acute Kidney Injury: The Impact of Preoperative Estimated GFR
- PMID: 26386737
- PMCID: PMC4658239
- DOI: 10.1053/j.ajkd.2015.07.027
Urine Biomarkers and Perioperative Acute Kidney Injury: The Impact of Preoperative Estimated GFR
Abstract
Background: The interaction between baseline kidney function and the performance of biomarkers of acute kidney injury (AKI) on the development of AKI is unclear.
Study design: Post hoc analysis of prospective cohort study.
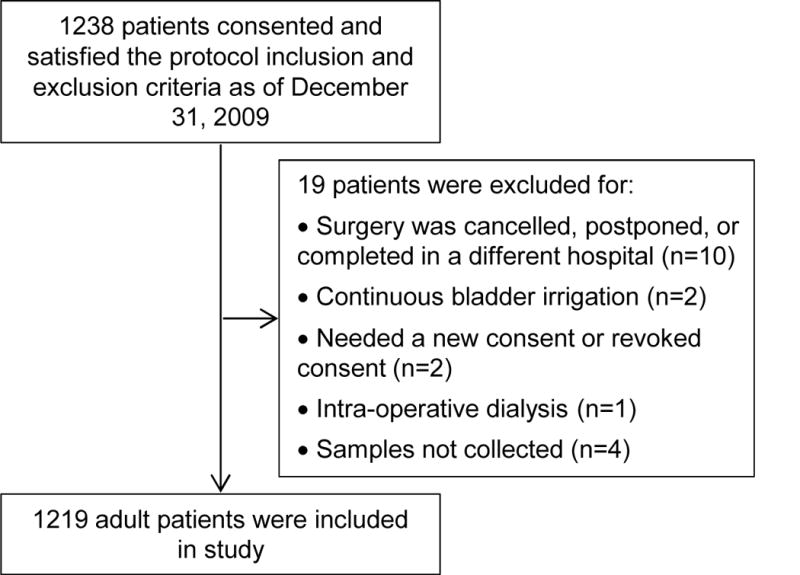
Setting & participants: The 1,219 TRIBE-AKI Consortium adult cardiac surgery cohort participants.
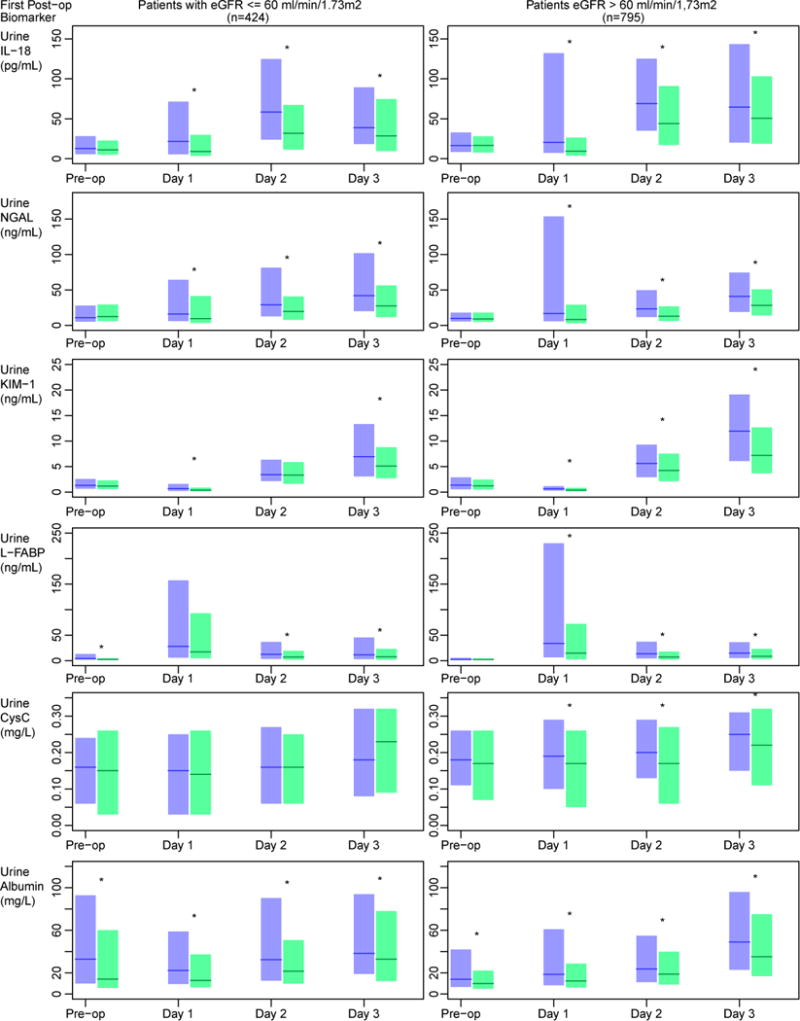
Predictor: Unadjusted postoperative urinary biomarkers of AKI measured within 6 hours of surgery.
Outcome: AKI was defined as AKI Network stage 1 (any AKI) or higher, as well as a doubling of serum creatinine level from the preoperative value or the need for post-operative dialysis (severe AKI).
Measurements: Stratified analyses by preoperative estimated glomerular filtration rate (eGFR) ≤ 60 versus > 60mL/min/1.73m(2).
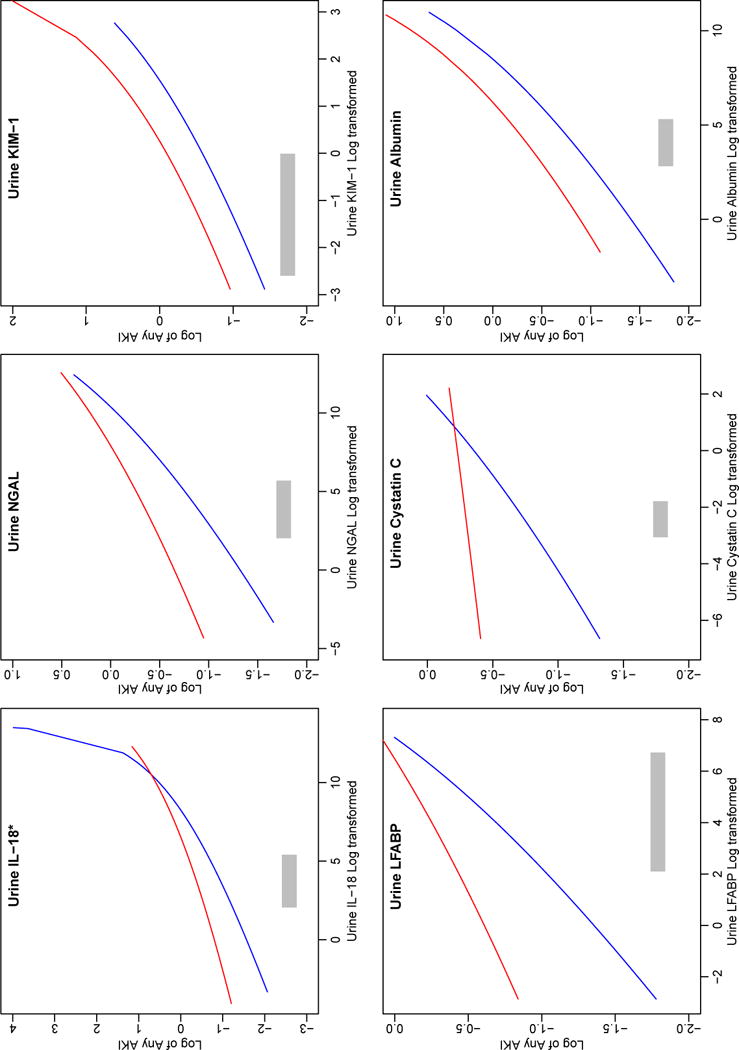
Results: 180 (42%) patients with preoperative eGFRs≤60mL/min/1.73m(2) developed clinical AKI compared with 246 (31%) of those with eGFRs>60mL/min/1.73m(2) (P<0.001). For log2-transformed biomarker concentrations, there was a significant interaction between any AKI and baseline eGFR for interleukin 18 (P=0.007) and borderline significance for liver-type fatty acid binding protein (P=0.06). For all biomarkers, the adjusted relative risk (RR) point estimates for the risk for any AKI were higher in those with elevated baseline eGFRs compared with those with eGFRs≤60mL/min/1.73m(2). However, the difference in magnitude of these risks was low (adjusted RRs were 1.04 [95% CI, 0.99-1.09] and 1.11 [95% CI, 1.07-1.15] for those with preoperative eGFRs≤60mL/min/1.73m(2) and those with higher eGFRs, respectively). Although no biomarker displayed an interaction for baseline eGFR and severe AKI, log2-transformed interleukin 18 and kidney injury molecule 1 had significant adjusted RRs for severe AKI in those with and without baseline eGFRs≤60mL/min/1.73m(2).
Limitations: Limited numbers of patients with severe AKI and post-operative dialysis.
Conclusions: The association between early postoperative AKI urinary biomarkers and AKI is modified by preoperative eGFR. The degree of this modification and its impact on the biomarker-AKI association is small across biomarkers. Our findings suggest that distinct biomarker cutoffs for those with and without a preoperative eGFR≤60mL/min/1.73m(2) is not necessary.
Keywords: Urine biomarkers; acute kidney injury (AKI); acute renal failure (ARF); cardiac surgery; effect modification; estimated glomerular filtration rate (eGFR); interleukin 18 (IL-18); liver-type fatty acid binding protein (L-FABP); perioperative AKI; prognosis; surgical complication.
Published by Elsevier Inc.
Figures
References
-
- Koyner JL, Cerda J, Goldstein SL, et al. The Daily Burden of Acute Kidney Injury: A World Kidney Day Survey of U.S. Nephrologists. Journal of the American Society of Nephrology. 2013;24:3A. Oral Abstract Presented at ASN Renal Week - Thursdayvember 7, 2013. - PubMed
-
- Koyner JL, Parikh CR. Clinical Utility of Biomarkers of AKI in Cardiac Surgery and Critical Illness. Clin J Am Soc Nephrol. 2013;8(6):1034–1042. - PubMed
-
- Bihorac A, Chawla LS, Shaw AD, et al. Validation of Cell-Cycle Arrest Biomarkers for Acute Kidney Injury Using Clinical Adjudication. Am J Respir Crit Care Med. 2014;189(8):932–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL085757/HL/NHLBI NIH HHS/United States
- K23DK081616/DK/NIDDK NIH HHS/United States
- K24DK090203/DK/NIDDK NIH HHS/United States
- P30 DK079310/DK/NIDDK NIH HHS/United States
- K23 DK080132/DK/NIDDK NIH HHS/United States
- R01HL085757/HL/NHLBI NIH HHS/United States
- K23 DK081616/DK/NIDDK NIH HHS/United States
- K23DK080132/DK/NIDDK NIH HHS/United States
- U01 DK082185/DK/NIDDK NIH HHS/United States
- K24 DK090203/DK/NIDDK NIH HHS/United States
- UL1 TR000430/TR/NCATS NIH HHS/United States
- U01DK082185/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
