

Evidence for the changing regimens of acetylcysteine
- PMID: 26387650
- PMCID: PMC4767192
- DOI: 10.1111/bcp.12789
Evidence for the changing regimens of acetylcysteine
Abstract
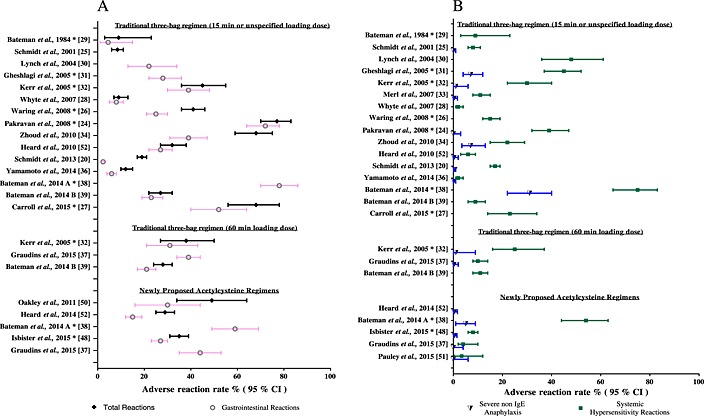
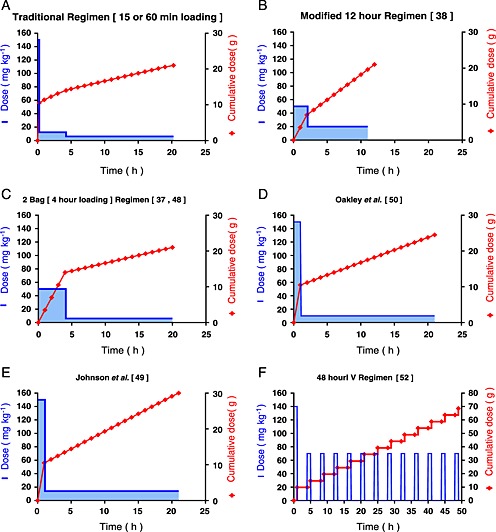
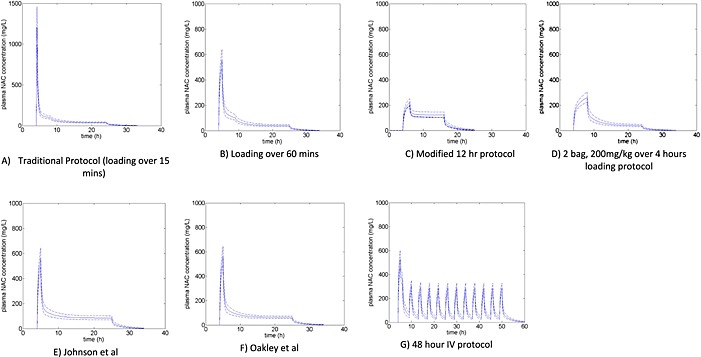
Paracetamol overdose prior to the introduction of acetylcysteine was associated with significant morbidity. Acetylcysteine is now the mainstay of treatment for paracetamol poisoning and has effectively reduced rates of hepatotoxicity and death. The current three-bag intravenous regimen with an initial high loading dose was empirically derived four decades ago and has not changed since. This regimen is associated with a high rate of adverse effects due mainly to the high initial peak acetylcysteine concentration. Furthermore, there are concerns that the acetylcysteine concentration is not adequate for 'massive' overdoses and that the dose and duration may need to be altered. Various novel regimens have been proposed, looking to address these issues. Many of these modified regimens aim to decrease the rate of adverse reactions by slowing the loading dose and thereby decrease the peak concentration. We used a published population pharmacokinetic model of acetylcysteine to simulate these modified regimens. We determined mean peak and 20 h acetylcysteine concentrations and area under the under the plasma concentration-time curve to compare these regimens. Those regimens that resulted in a lower peak acetylcysteine concentration have been shown in studies to have a lower rate of adverse events. However, these studies were too small to show whether they are as effective as the traditional regimen. Further research is still needed to determine the optimum dose and duration of acetylcysteine that results in the fewest side-effects and treatment failures. Indeed, a more patient-tailored approach might be required, whereby the dose and duration are altered depending on the paracetamol dose ingested or paracetamol concentrations.
Keywords: acetylcysteine; antidote; overdose; paracetamol.
© 2015 The British Pharmacological Society.
Figures
References
-
- Larson AM, Polson J, Fontana RJ, Davern TJ, Lalani E, Hynan LS, Reisch JS, Schiødt FV, Ostapowicz G, Shakil AO, Lee WM, Acute Liver Failure Study Group . Acetaminophen‐induced acute liver failure: results of a United States multicenter, prospective study. Hepatology 2005; 42: 1364–72. - PubMed
-
- Lancaster EM, Hiatt JR, Zarrinpar A. Acetaminophen hepatotoxicity: an updated review. Arch Toxicol 2015; 89: 193–9. - PubMed
-
- Rumack BH, Bateman DN. Acetaminophen and acetylcysteine dose and duration: past, present and future. Clin Toxicol 2012; 50: 91–8. - PubMed
-
- Hayes BD, Klein‐Schwartz W, Doyon S. Frequency of medication errors with intravenous acetylcysteine for acetaminophen overdose. Ann Pharmacother 2008; 42: 766–70. - PubMed
-
- Mitchell JR, Thorgeirsson SS, Potter WZ, Jollow DJ, Keiser H. Acetaminophen‐induced hepatic injury: protective role of glutathione in man and rationale for therapy. Clin Pharmacol Ther 1974; 16: 676–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
