

Understanding Decision Making in Critical Care
- PMID: 26387708
- PMCID: PMC4720506
- DOI: 10.3121/cmr.2015.1289
Understanding Decision Making in Critical Care
Abstract
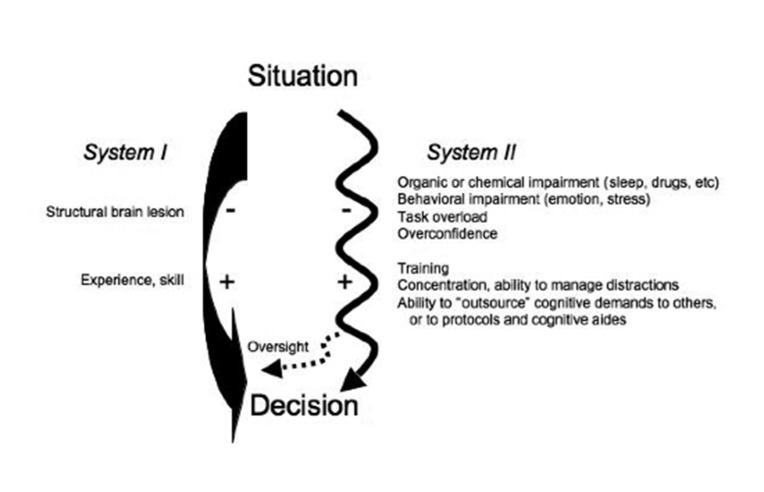
Background: Human decision making involves the deliberate formulation of hypotheses and plans as well as the use of subconscious means of judging probability, likely outcome, and proper action.
Rationale: There is a growing recognition that intuitive strategies such as use of heuristics and pattern recognition described in other industries are applicable to high-acuity environments in medicine. Despite the applicability of theories of cognition to the intensive care unit, a discussion of decision-making strategies is currently absent in the critical care literature.
Content: This article provides an overview of known cognitive strategies, as well as a synthesis of their use in critical care. By understanding the ways by which humans formulate diagnoses and make critical decisions, we may be able to minimize errors in our own judgments as well as build training activities around known strengths and limitations of cognition.
Keywords: Critical care; Diagnosis; Heuristics; Intuition; Medical decision making.
© 2015 Marshfield Clinic.
Figures
References
-
- Croskerry P, Norman G. Overconfidence in clinical decision making. Am J Med 2008;121:S24–S29. - PubMed
-
- Berner ES, Graber ML. Overconfidence as a cause of diagnostic error in medicine. Am J Med 2008;121:S2–S23. - PubMed
-
- Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, Lawthers AG, Newhouse JP, Weiler PC, Hiatt HH. Incidence of adverse events and negligence in hospitalized patients: results of the Harvard Medical Practice Study I. N Engl J Med 1991;324:370–376. - PubMed
-
- Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, Hebert L, Newhouse JP, Weiler PC, Hiatt H. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med 1991;324:377–384. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical