

Review
doi: 10.1038/nri3887.
Epub 2015 Sep 21.
The nature of immune responses to urinary tract infections
Affiliations
- PMID: 26388331
- PMCID: PMC4926313
- DOI: 10.1038/nri3887
Item in Clipboard
Review
The nature of immune responses to urinary tract infections
Nat Rev Immunol.
2015 Oct.
Abstract
The urinary tract is constantly exposed to microorganisms that inhabit the gastrointestinal tract, but generally the urinary tract resists infection by gut microorganisms. This resistance to infection is mainly ascribed to the versatility of the innate immune defences in the urinary tract, as the adaptive immune responses are limited particularly when only the lower urinary tract is infected. In recent years, as the strengths and weaknesses of the immune system of the urinary tract have emerged and as the virulence attributes of uropathogens are recognized, several potentially effective and unconventional strategies to contain or prevent urinary tract infections have emerged.
Figures
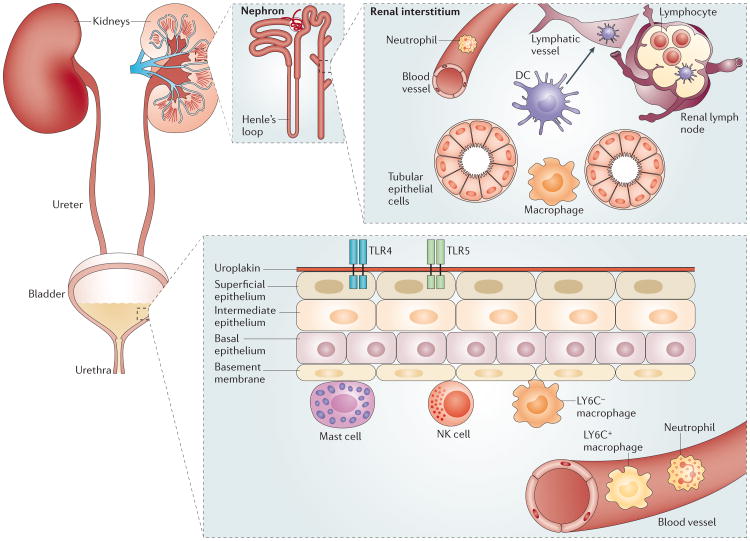
A variety of cell types are responsible for initiating immune responses along the urinary tract. The upper urinary tract is comprised primarily of the kidneys, and the filtration function of the kidneys is performed by hundreds of thousands of nephrons, each of which is composed of a glomerulus and a double hairpin-shaped tubule. Many of the immune-competent cells, including dendritic cells (DCs) and macrophages, are aggregated in the interstitium in close proximity to both the tubular epithelium and blood vessels. In addition, there is a large network of lymphatic vessels in these organs, which connects to the renal lymph nodes. The ureters, urethra and bladder constitute the lower urinary tract, and several layers of stratified epithelial cells that line the bladder function as the first line of defence. The major resident immune cells in the bladder include mast cells and LY6C− macrophages. These cells are located underneath the basal epithelium and function as sentinels to sense infection and recruit neutrophils and LY6C+ macrophages from the bladder. NK, natural killer; TLR, Toll-like receptor.
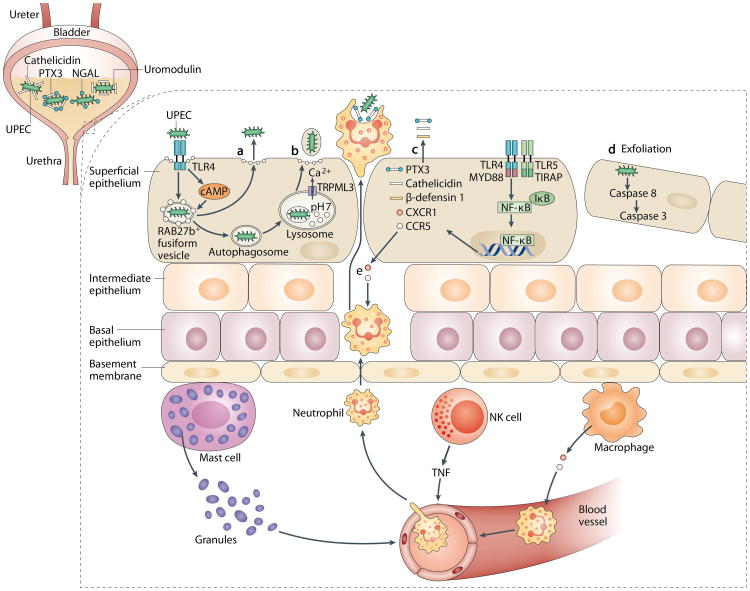
A robust and complicated network of innate immune responses can be initiated in the bladder in response to infection. a | Following invasion by uropathogenic Escherichia coli (UPEC) and encapsulation within RAB27b+ vesicles in bladder epithelial cells (BECs), Toll-like receptor 4 (TLR4) recognizes intracellular UPEC and increases intracellular cyclic AMP (cAMP) levels. This leads to exocytosis of RAB27b+ vesicles harbouring UPEC and expulsion of the intracellular UPEC back into the lumen of the bladder. b | When intracellular UPEC escape the first wave of expulsion by breaking the RAB27b+ vacuole, these bacteria are targeted by autophagy and delivered into the lysosomes, which in turn are manipulated by UPEC to lose their degradative capacity. These malfunctioning lysosomes are sensed by a lysosomal transient receptor potential (TRP) mucolipin 3 channel (TRPML3) and trigger lysosome exocytosis, resulting in bacterial expulsion. c | Upon sensing the presence of pathogens by TLR4 and subsequent signalling a wide range of soluble factors are also secreted by BECs, including antimicrobial peptides (such as cathelicidin and β-defensin 1), antimicrobial proteins (such as pentraxin 3 (PTX3)) and chemokines (such as CXCL1 and CCL5). d| Bacterial infection initiates caspase 3-and caspase 8-dependent apoptosis of infected BECs, which shed into the bladder lumen; this represents another effective mechanism to reduce bacterial load. e | Coordinated cellular immune responses in the bladder are shown. The resident sentinel immune cells — such as mast cells, natural killer (NK) cells and macrophages — can sense the presence of the infections and secrete various cytokines to recruit other innate immune cells from the bloodstream, especially neutrophils to clear the infections. IκB, NF-κB inhibitor; MYD88, myeloid differentiation primary response protein 88;NGAL, neutrophil gelatinase-associated lipocalin; NF-κB, nuclear factor-κB; TIRAP, Toll/IL-1R domain-containing adaptor protein; TNF, tumour necrosis factor.
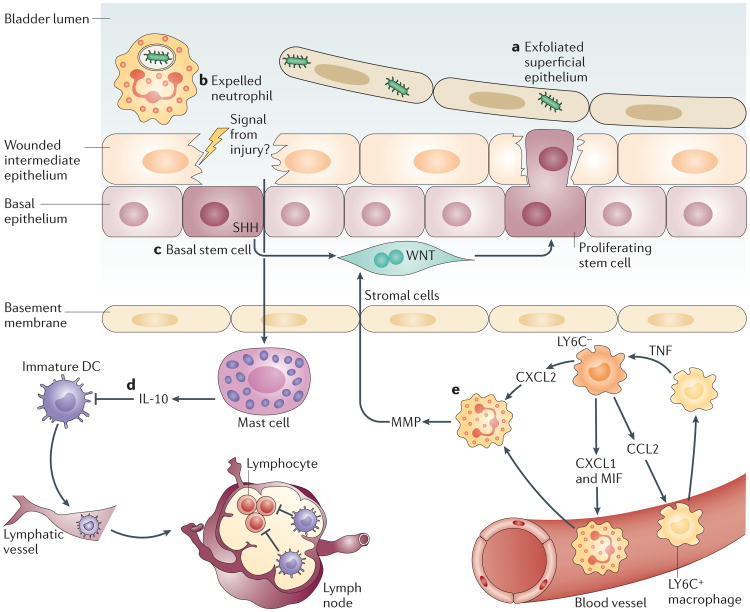
Infections of the superficial epithelium can eventually lead to extensive exfoliation of bladder epithelial cells (part a), resulting in loss of the physical barrier. Each type of immune cell possesses specialized strategies to prevent excessive inflammation and to maintain the tissue integrity. Neutrophils are rapidly expelled into the urine, possibly to reduce the tissue damage from their toxic granules (part b). Local stem cells and stromal cells underneath the intermediate epithelium sense damage to the tissue and initiate a proliferation programme to regenerate the tissue barrier (part c). Local mast cells, which were previously active in mediating a pro-inflammatory immune response, sense the damaged epithelium and switch to mediating anti-inflammatory responses to facilitate regeneration of the epithelium (part d). This switch in activity is achieved by secreting large amount of interleukin-10 (IL-10). Local IL-10 suppresses the activation of dendritic cells (DCs) but not their migration to the iliac lymph nodes. Immature DCs are unable to induce substantial antibody responses in the lymph nodes. Intimate crosstalk between LY6C− and LY6C+ macrophages provides a ‘double-safe’ checkpoint to ensure precise initiation of neutrophil responses (part e): local LY6C− macrophages release CC-chemokine ligand 2 (CCL2), chemokine CXC-chemokine ligand 1 (CXCL1) and macrophage migration inhibitory factor (MIF) to recruit LY6C+ macrophages and neutrophils from the bloodstream. Upon sensing the infection, LY6C+ macrophages secrete tumour necrosis factor (TNF), which acts on local LY6C− macrophages to trigger their production of CXCL2, which induces neutrophils to cross the basal membrane. MMP, matrix metalloproteinase; SHH, sonic hedgehog.
References
-
- Grist M, Chakraborty J. Identification of a mucin layer in the urinary bladder. Urology. 1994;44:26–33. - PubMed
-
- Ronald A. The etiology of urinary tract infection: traditional and emerging pathogens. Am J Med. 2002;113(Suppl. 1A):14S–19S. - PubMed
-
- Foxman B, Barlow R, D'Arcy H, Gillespie B, Sobel JD. Urinary tract infection: self-reported incidence and associated costs. Ann Epidemiol. 2000;10:509–515. - PubMed
-
- Schaeffer AJ. Recurrent urinary tract infections in women. Pathogenesis and management. Postgrad Med. 1987;81:51–58. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
