

Failure of Flow Diverter Treatment of Intracranial Aneurysms Related to the Fetal-type Posterior Communicating Artery
- PMID: 26389008
- PMCID: PMC4571555
- DOI: 10.5469/neuroint.2015.10.2.60
Failure of Flow Diverter Treatment of Intracranial Aneurysms Related to the Fetal-type Posterior Communicating Artery
Abstract
Purpose: The pipeline embolization device (PED) is a flow diverter that has shown promise in the treatment of intracranial aneurysms. Close to one-fifth of aneurysms, however, fail to occlude after PED placement. This study aims to identify anatomical features and clinicopathologic factors that may predispose failed aneurysm occlusion with the PED.
Materials and methods: We retrospectively reviewed all anterior circulation unruptured saccular aneurysms treated with the PED in a single-center. The primary outcome measure was angiographic occlusion. Anatomical features and potential predictors, including gender, aneurysm location, size, height, aspect ratio, neck width, prior treatment and the number of PED, were studied using binary logistic regression.
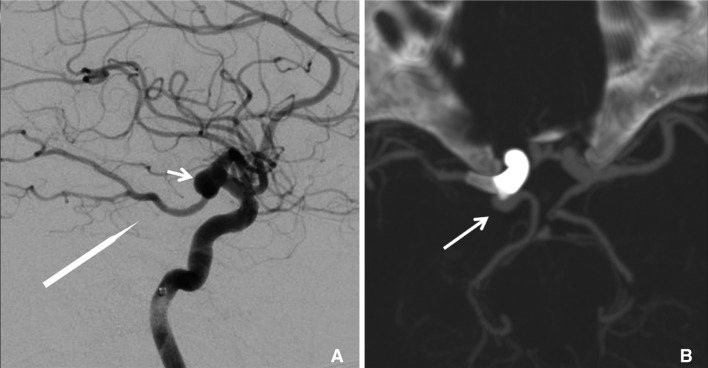
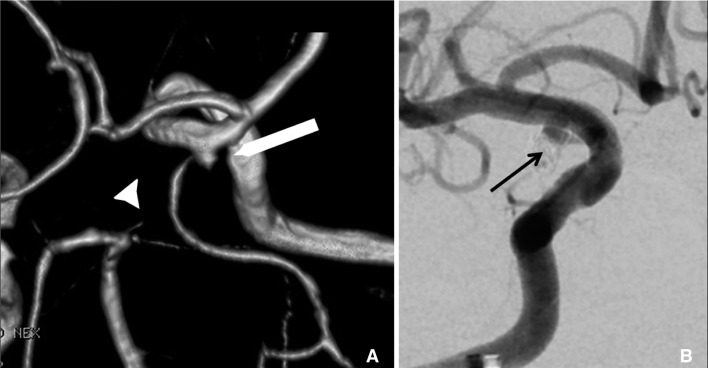
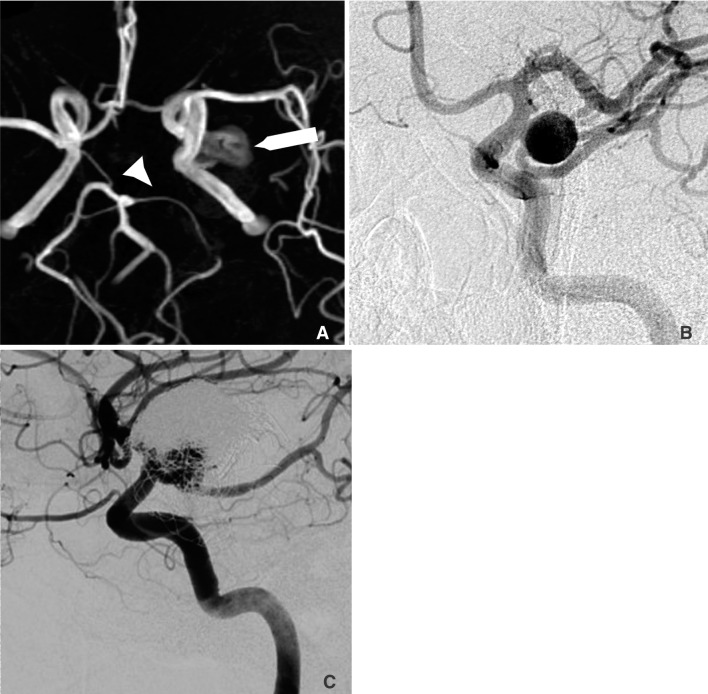
Results: 29 anterior circulation unruptured saccular aneurysms with a mean size of 6.99 mm treated with the PED in a single center were retrospectively studied. The overall occlusion rate was 79.3% after a mean follow-up of 9.2 months. Four aneurysms were related to the fetal-type posterior communicating artery (PComA), and all were refractory to flow diverter treatment. Female gender was significantly associated with a higher occlusion rate. We present the anatomical features and propose possible pathophysiological mechanisms of these PComA aneurysms that failed flow diverter treatment.
Conclusion: A PComA aneurysm with persistent fetal-type circulation appears to be particularly refractory to flow diverter treatment, especially when the aneurysm incorporates a significant portion of the PComA. Our experience suggested that flow diverting stents alone may not be the ideal treatment for this subgroup of aneurysms, and alternative modalities should be considered. Female patients were found to have a significantly higher rate of treatment success.
Keywords: Fetal circulation; Flow diverters; Intracranial aneurysm; Outcome; Pipeline embolization device.
Figures
References
-
- Fiorella D, Kelly ME, Albuquerque FC, Nelson PK. Curative reconstruction of a giant midbasilar trunk aneurysm with the pipeline embolization device. Neurosurgery. 2009;64:212–217. - PubMed
-
- Fiorella D, Woo HH, Albuquerque FC, Nelson PK. Definitive reconstruction of circumferential, fusiform intracranial aneurysms with the pipeline embolization device. Neurosurgery. 2008;62:1115–1120. - PubMed
-
- Lylyk P, Miranda C, Ceratto R, Ferrario A, Scrivano E, Luna HR, et al. Curative endovascular reconstruction of cerebral aneurysms with the pipeline embolization device: the Buenos Aires experience. Neurosurgery. 2009;64:632–642. - PubMed
-
- Yu SC, Kwok CK, Cheng PW, Chan KY, Lau SS, Lui WM, et al. Intracranial aneurysms: midterm outcome of pipeline embolization device--a prospective study in 143 patients with 178 aneurysms. Radiology. 2012;265:893–901. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
