

Do Lower Target Temperatures or Prolonged Cooling Provide Improved Outcomes for Comatose Survivors of Cardiac Arrest Treated With Hypothermia?
- PMID: 26391133
- PMCID: PMC4599499
- DOI: 10.1161/JAHA.115.002123
Do Lower Target Temperatures or Prolonged Cooling Provide Improved Outcomes for Comatose Survivors of Cardiac Arrest Treated With Hypothermia?
Abstract
Background: Optimal protocols for targeted temperature management are still unclear. This study investigated whether lower target temperatures and/or prolonged cooling could provide improved outcomes in comatose survivors of cardiac arrest.
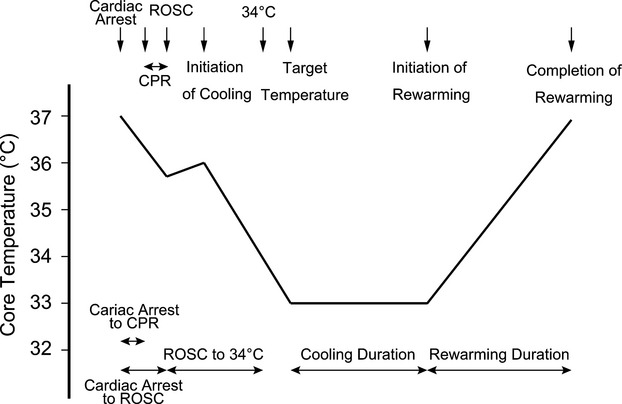
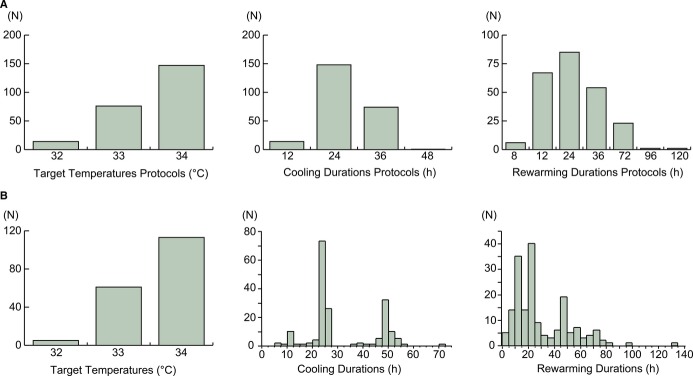
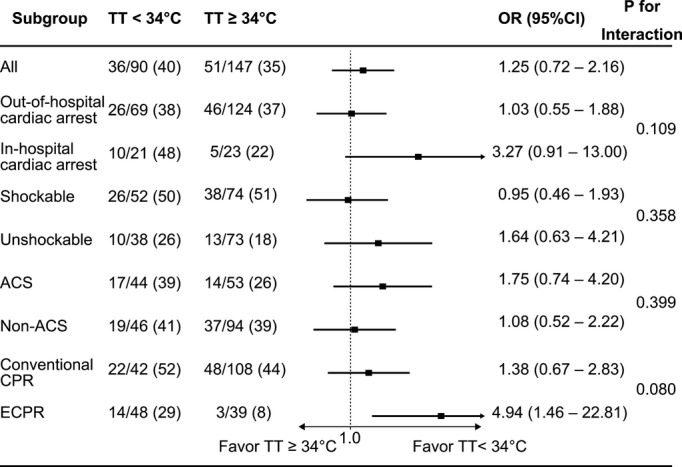
Methods and results: This observational study was conducted using the prospectively collected targeted temperature management database in Hiroshima, Japan. Between September 2003 and September 2014, 237 patients treated with TTM after cardiac arrest were enrolled in this study. The target temperatures and durations were assigned by the treating physicians regardless of the patients' conditions. Favorable outcomes were defined as a cerebral performance category scale of 1 or 2 at the 90-day follow-up time point. The rate of favorable outcomes were similar between the patients whose protocols of target temperature were <34°C and ≥34°C (40% versus 35%, P=0.41), cooling durations were <28 and ≥28 hours (33% versus 44%, P=0.11), and rewarming durations were <28 and ≥28 hours (35% versus 41%, P=0.39). However, in patients treated with extracorporeal cardiopulmonary resuscitation, target temperatures <34°C were associated with more favorable outcomes (29% versus 8%, P=0.01). The cooling and rewarming durations >28 hours and target temperatures <34°C were associated with more frequent lethal arrhythmia, pneumonia, and/or bleedings.
Conclusions: Prolonged durations of cooling and rewarming ≥28 hours may not improve outcomes and may increase complications. Further studies are necessary to assess the hypothesis that target temperatures <34°C provide improved outcomes in patients treated with extracorporeal cardiopulmonary resuscitation.
Keywords: cardiopulmonary resuscitation; extracorporeal circulation; heart arrest; targeted temperature management; therapeutic hypothermia.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Safar P. Cerebral resuscitation after cardiac arrest: research initiatives and future directions. Ann Emerg Med. 1993;22:324–349. - PubMed
-
- Kitamura T, Iwami T, Kawamura T, Nagao K, Tanaka H, Hiraide A. Nationwide public-access defibrillation in Japan. N Engl J Med. 2010;362:994–1004. - PubMed
-
- Booth CM, Boone RH, Tomlinson G, Detsky AS. Is this patient dead, vegetative, or severely neurologically impaired? Assessing outcome for comatose survivors of cardiac arrest. JAMA. 2004;291:870–879. - PubMed
-
- The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
