

Impact of Contact Force Technology on Atrial Fibrillation Ablation: A Meta-Analysis
- PMID: 26391136
- PMCID: PMC4599513
- DOI: 10.1161/JAHA.115.002476
Impact of Contact Force Technology on Atrial Fibrillation Ablation: A Meta-Analysis
Abstract
Background: Catheter-tissue contact is essential for effective lesion formation, thus there is growing usage of contact force (CF) technology in atrial fibrillation ablation. We conducted a meta-analysis to assess the impact of CF on clinical outcomes and procedural parameters in comparison to conventional catheter for atrial fibrillation ablation.
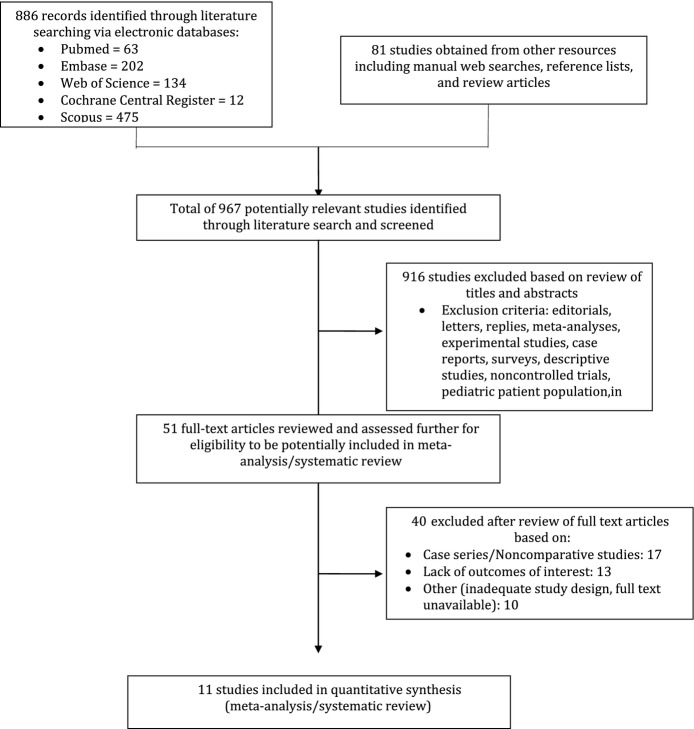
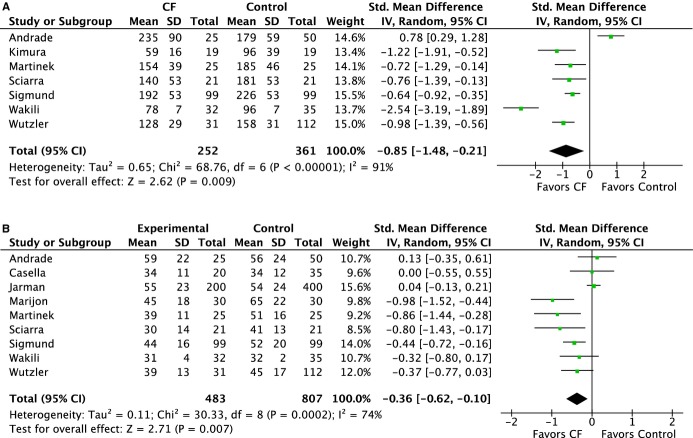
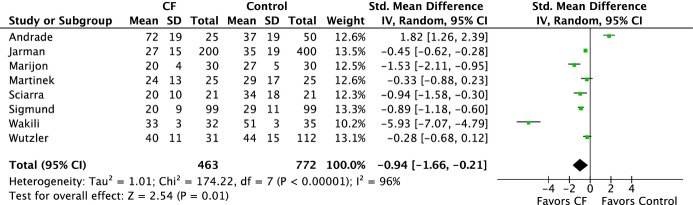
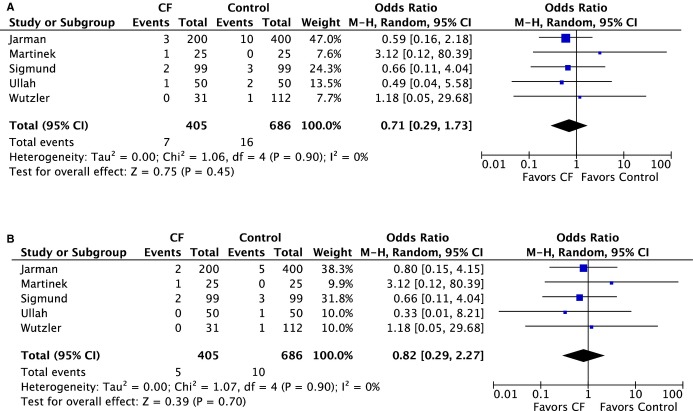
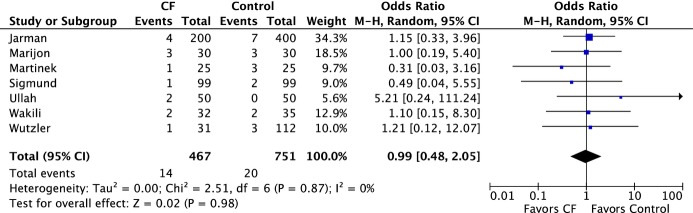
Methods and results: An electronic search was performed using major databases. Outcomes of interest were recurrence rate, major complications, total procedure, and fluoroscopic times. Continuous variables were reported as standardized mean difference; odds ratios were reported for dichotomous variables. Eleven studies (2 randomized controlled studies and 9 cohorts) involving 1428 adult patients were identified. CF was deployed in 552 patients. The range of CF used was between 2 to 60 gram-force. The follow-up period ranged between 10 and 53 weeks. In comparing CF and conventional catheter groups, the recurrence rate was lower with CF (35.1% versus 45.5%, odds ratio 0.62 [95% CI 0.45-0.86], P=0.004). Shorter procedure and fluoroscopic times were achieved with CF (procedure time: 156 versus 173 minutes, standardized mean difference -0.85 [95% CI -1.48 to -0.21], P=0.009; fluoroscopic time: 28 versus 36 minutes, standardized mean difference -0.94 [95% CI -1.66; -0.21], P=0.01). Major complication rate was lower numerically in the CF group but not statistically significant (1.3% versus 1.9%, odds ratio 0.71 [95% CI 0.29-1.73], P=0.45).
Conclusions: The use of CF technology results in significant reduction of the atrial fibrillation recurrence rate after atrial fibrillation ablation in comparison to the conventional catheter group. CF technology is able to significantly reduce procedure and fluoroscopic times without compromising complication rate.
Keywords: ablation; atrial fibrillation; contact force; meta‐analysis.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures

References
-
- Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, D’Agostino RB, Massaro JM, Beiser A, Wolf PA, Benjamin EJ. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110:1042–1046. - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW Members AATF. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104. - PubMed
-
- Shurrab M, Fishman E, Kaoutskaia A, Birnie D, Ayala-Paredes F, Sultan O, Chauhan V, Skanes A, Parkash R, Morillo C, Janmohamed A, Toal S, Essebag V, Sterns L, Veenhuyzen G, Mangat I, Redfearn D, Philippon F, Connors S, Healey J, Verma A, Crystal E. Snapshot of adult invasive cardiac electrophysiology in Canada: results of the web-based registry. J Interv Card Electrophysiol. 2014;40:93–98. - PubMed
-
- Cappato R, Negroni S, Pecora D, Bentivegna S, Lupo PP, Carolei A, Esposito C, Furlanello F, De Ambroggi L. Prospective assessment of late conduction recurrence across radiofrequency lesions producing electrical disconnection at the pulmonary vein ostium in patients with atrial fibrillation. Circulation. 2003;108:1599–1604. - PubMed
-
- Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, Skanes A. Prevalence and causes of fatal outcome in catheter ablation of atrial fibrillation. J Am Coll Cardiol. 2009;53:1798–1803. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
