

Could caregiver reporting adherence help detect virological failure in Cameroonian early treated HIV-infected infants?
- PMID: 26391474
- PMCID: PMC4578260
- DOI: 10.1186/s12887-015-0451-3
Could caregiver reporting adherence help detect virological failure in Cameroonian early treated HIV-infected infants?
Abstract
Background: Viral load is still the marker of choice for monitoring adherence to combined antiretroviral therapy (cART) and confirming the success of HIV treatment. Unfortunately it is difficult to access in many resource-poor settings. We aimed to measure the performance of caregiver reporting adherence for detecting virological failure in routine practice during the first 2 years after cART initiation in infants.
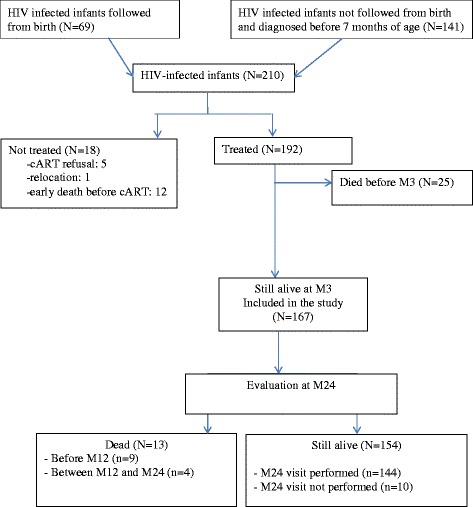
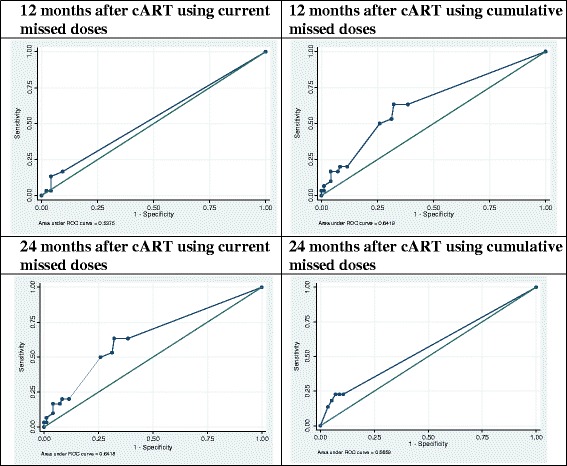
Methods: PEDIACAM is an ongoing prospective cohort study including HIV1-infected infants diagnosed before 7 months of age between November 2007 and October 2011 in Cameroon. Adherence was assessed using a questionnaire administered every 3 months from cART initiation; the HIV-RNA viral load was determined at the same visits. Virological failure was defined as having a viral load ≥ 1000 cp/mL at 3 and 12 months after cART initiation or having a viral load ≥ 400 cp/mL at 24 months after cART initiation. The performance of each current missed and cumulative missed dose defined according to adherence as reported by caregiver was assessed using the viral load as the gold standard.
Results: cART was initiated at a median age of 4 months (IQR: 3-6) in the 167 infants included. The cumulative missed dose showed the best overall performance for detecting virological failure after 12 months of cART (AUC test, p = 0.005, LR + =4.4 and LR- = 0.4). Whatever the adherence reporting criterion, the negative predictive value was high (NPV ≥ 75%) 12 and 24 months after cART initiation, whereas the positive predictive value was low (PPV ≤ 50%).
Conclusions: The adherence questionnaire administered by the health care provider to the infants' caregivers is not reliable for detecting virological failure in routine practice: its positive predictive value is low. However, the cumulative missed dose measurement may be a reliable predictor of virological success, particularly after 12 months of cART, given its high negative predictive value.
Figures
References
-
- Hainline C, Taliep R, Sorour G, Nachman S, Rabie H, Dobbels E, et al. Early Antiretroviral Therapy reduces the incidence of otorrhea in a randomized study of early and deferred antiretroviral therapy: Evidence from the Children with HIV Early Antiretroviral Therapy (CHER) Study. BMC Res Notes. 2011;4:448. doi: 10.1186/1756-0500-4-448. - DOI - PMC - PubMed
-
- Van Rossum A, Geelen S, Hartwig N, Wolfs T, Weemaes C, Sherpbier H, et al. Results of 2 years of treatment with protease-inhibitor-containing antiretroviral therapy in dutch children infected with human immunodeficiency virus type I. Clin Infect Dis. 2002;34(7):1008–16. doi: 10.1086/339443. - DOI - PubMed
-
- Doherty M, Ford N, Vitoria M, Weiler G, Hirnschall G. The 2013 WHO guidelines for antiretroviral therapy: evidence-based recommendations to face new epidemic realities. HIV Department, World Health Organization, Geneva, Switzerland. Curr Opin HIV AIDS. 2013;8(6):528–34. doi: 10.1097/COH.0000000000000008. - DOI - PubMed
-
- UNICEF . A call to action: children the missing face of AIDS. New York: UNAIDS; 2005.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
