

Association of Intensive Care Unit Admission With Mortality Among Older Patients With Pneumonia
- PMID: 26393850
- PMCID: PMC4758179
- DOI: 10.1001/jama.2015.11068
Association of Intensive Care Unit Admission With Mortality Among Older Patients With Pneumonia
Erratum in
-
Incorrect Affiliation.JAMA. 2015 Nov 17;314(19):2086. doi: 10.1001/jama.2015.14004. JAMA. 2015. PMID: 26575073 No abstract available.
Abstract
Importance: Among patients whose need for intensive care is uncertain, the relationship of intensive care unit (ICU) admission with mortality and costs is unknown.
Objective: To estimate the relationship between ICU admission and outcomes for elderly patients with pneumonia.
Design, setting, and patients: Retrospective cohort study of Medicare beneficiaries (aged >64 years) admitted to 2988 acute care hospitals in the United States with pneumonia from 2010 to 2012.
Exposures: ICU admission vs general ward admission.
Main outcomes and measures: Primary outcome was 30-day all-cause mortality. Secondary outcomes included Medicare spending and hospital costs. Patient and hospital characteristics were adjusted to account for differences between patients with and without ICU admission. To account for unmeasured confounding, an instrumental variable was used-the differential distance to a hospital with high ICU admission (defined as any hospital in the upper 2 quintiles of ICU use).
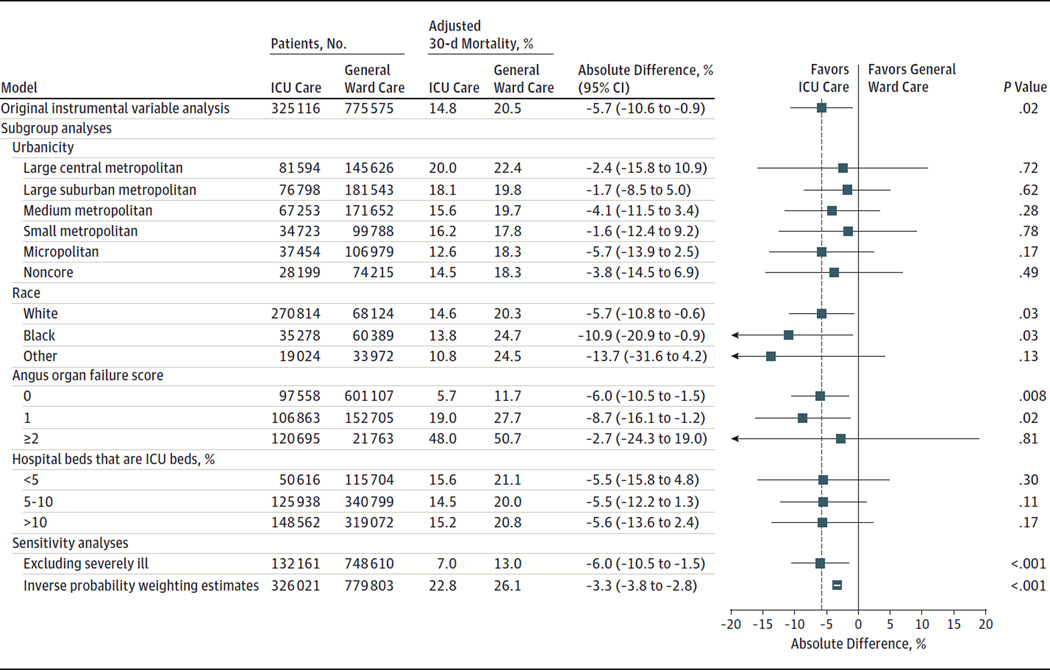
Results: Among 1,112,394 Medicare beneficiaries with pneumonia, 328,404 (30%) were admitted to the ICU. In unadjusted analyses, patients admitted to the ICU had significantly higher 30-day mortality, Medicare spending, and hospital costs than patients admitted to a general hospital ward. Patients (n = 553,597) living closer than the median differential distance (<3.3 miles) to a hospital with high ICU admission were significantly more likely to be admitted to the ICU than patients living farther away (n = 558,797) (36% for patients living closer vs 23% for patients living farther, P < .001). In adjusted analyses, for the 13% of patients whose ICU admission decision appeared to be discretionary (dependent only on distance), ICU admission was associated with a significantly lower adjusted 30-day mortality (14.8% for ICU admission vs 20.5% for general ward admission, P = .02; absolute decrease, -5.7% [95% CI, -10.6%, -0.9%]), yet there were no significant differences in Medicare spending or hospital costs for the hospitalization.
Conclusions and relevance: Among Medicare beneficiaries hospitalized with pneumonia, ICU admission of patients for whom the decision appeared to be discretionary was associated with improved survival and no significant difference in costs. A randomized trial may be warranted to assess whether more liberal ICU admission policies improve mortality for patients with pneumonia.
Conflict of interest statement
Figures
Comment in
-
Assessing the Value of Intensive Care.JAMA. 2015 Sep 22-29;314(12):1240-1. doi: 10.1001/jama.2015.11171. JAMA. 2015. PMID: 26393846 No abstract available.
-
Borderline pneumonia patients may benefit from intensive care, study finds.BMJ. 2015 Sep 23;351:h5017. doi: 10.1136/bmj.h5017. BMJ. 2015. PMID: 26403359 No abstract available.
-
Intensive Care Unit Admission and Mortality Among Medicare Beneficiaries With Pneumonia.JAMA. 2016 Mar 22-29;315(12):1284-5. doi: 10.1001/jama.2015.18020. JAMA. 2016. PMID: 27002453 No abstract available.
-
Intensive Care Unit Admission and Mortality Among Medicare Beneficiaries With Pneumonia--Reply.JAMA. 2016 Mar 22-29;315(12):1285. doi: 10.1001/jama.2015.18032. JAMA. 2016. PMID: 27002455 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
