

Procalcitonin Identifies Cell Injury, Not Bacterial Infection, in Acute Liver Failure
- PMID: 26393924
- PMCID: PMC4579124
- DOI: 10.1371/journal.pone.0138566
Procalcitonin Identifies Cell Injury, Not Bacterial Infection, in Acute Liver Failure
Abstract
Background: Because acute liver failure (ALF) patients share many clinical features with severe sepsis and septic shock, identifying bacterial infection clinically in ALF patients is challenging. Procalcitonin (PCT) has proven to be a useful marker in detecting bacterial infection. We sought to determine whether PCT discriminated between presence and absence of infection in patients with ALF.
Method: Retrospective analysis of data and samples of 115 ALF patients from the United States Acute Liver Failure Study Group randomly selected from 1863 patients were classified for disease severity and ALF etiology. Twenty uninfected chronic liver disease (CLD) subjects served as controls.
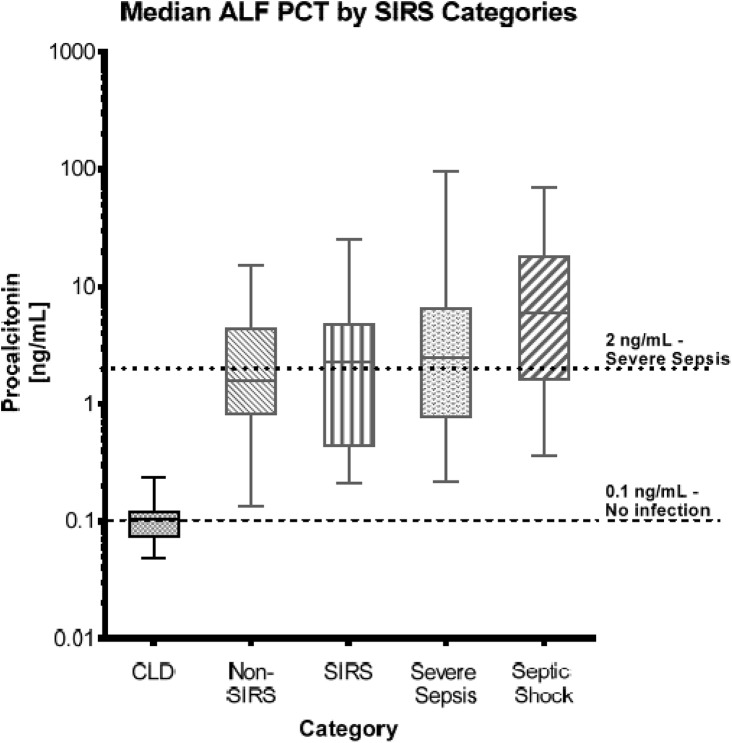
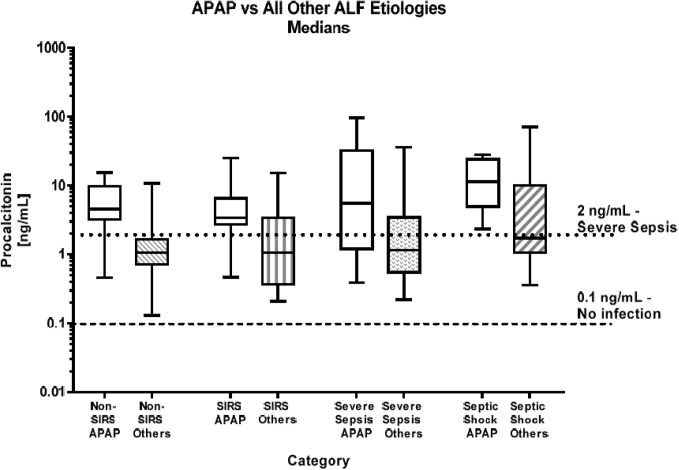
Results: Procalcitonin concentrations in most samples were elevated, with median values for all ALF groups near or above a 2.0 ng/mL cut-off that generally indicates severe sepsis. While PCT concentrations increased somewhat with apparent liver injury severity, there were no differences in PCT levels between the pre-defined severity groups-non-SIRS and SIRS groups with no documented infections and Severe Sepsis and Septic Shock groups with documented infections, (p = 0.169). PCT values from CLD patients differed from all ALF groups (median CLD PCT value 0.104 ng/mL, (p ≤0.001)). Subjects with acetaminophen (APAP) toxicity, many without evidence of infection, demonstrated median PCT >2.0 ng/mL, regardless of SIRS features, while some culture positive subjects had PCT values <2.0 ng/mL.
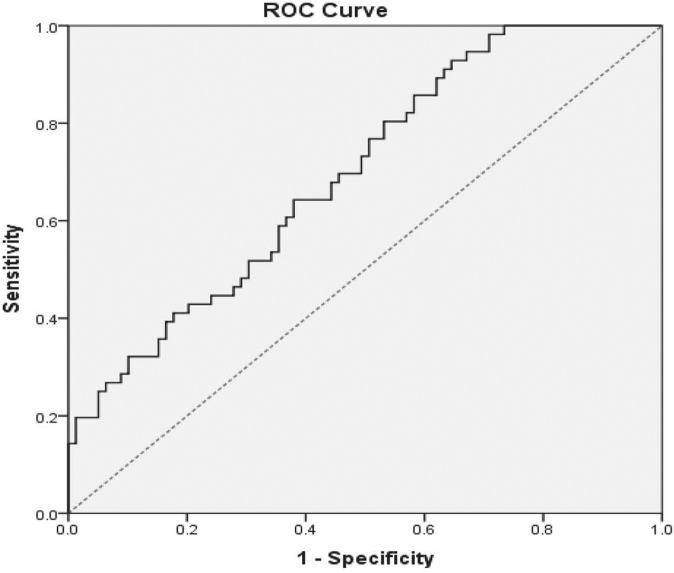
Summary/conclusions: While PCT appears to be a robust assay for detecting bacterial infection in the general population, there was poor discrimination between ALF patients with or without bacterial infection presumably because of the massive inflammation observed. Severe hepatocyte necrosis with inflammation results in elevated PCT levels, rendering this biomarker unreliable in the ALF setting.
Conflict of interest statement
Figures
References
-
- Rolando N, Wade J, Davalos M, Wendon J, Philpott-Howard J, Williams R. The systemic inflammatory response syndrome in acute liver failure. Hepatology, 2000; 32(4): 734–739. - PubMed
-
- Rolando N, Wade J, Davalos M, Wendon J, Philpott-Howard J, Williams R. Timing and aetiology of bacterial infections in a liver intensive care unit. J Hosp Infect, 2003; 53(2): 144–146. - PubMed
-
- Vaquero J, Polson J, Chung C, Helenowski I, Schiodt FV, Reisch J, et al. Infection and the progression of hepatic encephalopathy in acute liver failure. Gastroenterology, 2003; 125(3): 755–764. - PubMed
-
- Becker KL, Nylen ES, White JC, Muller B, Snider RH, Jr. Procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: A journey from calcitonin back to its precursors. J Clin Endocrinol Metab, 2004; 89(4): 1512–1525. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
