

What is the learning curve for the anterior approach for total hip arthroplasty?
- PMID: 26394641
- PMCID: PMC4626490
- DOI: 10.1007/s11999-015-4565-6
What is the learning curve for the anterior approach for total hip arthroplasty?
Abstract
Background: There are many factors that may affect the learning curve for total hip arthroplasty (THA) and surgical approach is one of these. There has been renewed interest in the direct anterior approach for THA with variable outcomes reported, but few studies have documented a surgeon's individual learning curve when using this approach.
Questions/purposes: (1) What was the revision rate for all surgeons adopting the anterior approach for placement of a particular implant? (2) What was the revision rate for surgeons who performed > 100 cases in this fashion? (3) Is there a minimum number of cases required to complete a learning curve for this procedure?
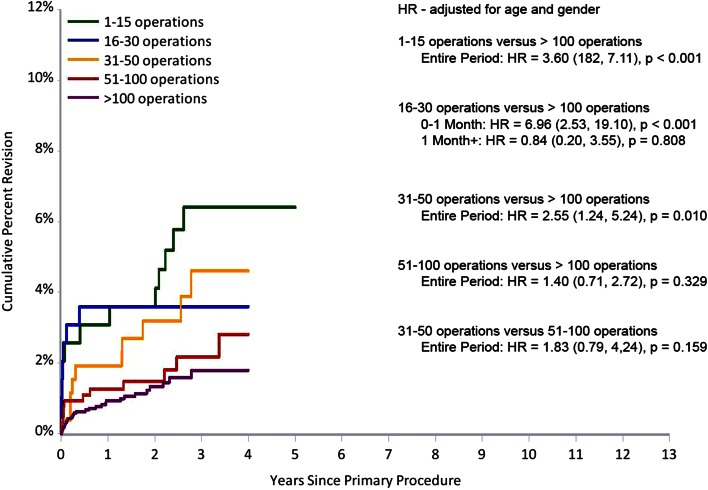
Methods: The Australian Orthopaedic Association National Joint Replacement Registry prospectively collects data on all primary and revision joint arthroplasty surgery. We analyzed all conventional THAs performed up to December 31, 2013, with a primary diagnosis of osteoarthritis using a specific implant combination and secondarily those associated with surgeons performing more than 100 procedures. Ninety-five percent of these procedures were performed through the direct anterior approach. Procedures using this combination were ordered from earliest (first procedure date) to latest (last procedure date) for each individual surgeon. Using the order number for each surgeon, five operation groups were defined: one to 15 operations, 16 to 30 operations, 31 to 50 operations, 51 to 100 operations, and > 100 operations. The primary outcome measure was time to first revision using Kaplan-Meier estimates of survivorship.
Results: Sixty-eight surgeons performed 5499 THAs using the specified implant combination. The cumulative percent revision at 4 years for all 68 surgeons was 3% (95% confidence interval [CI], 2.5-3.8). For surgeons who had performed over 100 operations, the cumulative revision rate was 3% (95% CI, 2.0-3.5). It was not until surgeons had performed over 50 operations that there was no difference in the cumulative percent revision compared with over 100 operations. The cumulative percent revision for surgeons performing 51 to 100 operations at 4 years was 3% (95% CI, 1.5-5.4) and over 100 operations 2% (95% CI, 1.2-2.7; hazard ratio, 1.40 [95% CI, 0.7-2.7]; p = 0.33).
Conclusions: There is a learning curve for the anterior approach for THA even when using a prosthesis combination specifically marketed for that approach. We found that 50 or more procedures need to be performed by a surgeon before the rate of revision is no different from performing 100 or more procedures. Surgeons should be aware of this initial higher rate of revision when deciding which approach delivers the best outcome for their patients.
Figures
References
-
- Australian Orthopaedic Association National Joint Replacement Registry Annual Report. Adelaide, Australia: AOA; 2009. Available at: https://aoanjrr.dmac.adelaide.edu.au/annual-reports-2009. Accessed February 2, 2015.
-
- Australian Orthopaedic Association National Joint Replacement Registry Annual Report. Adelaide, Australia :AOA; 2012. Available at: https://aoanjrr.dmac.adelaide.edu.au/annual-reports-2012. Accessed February 2, 2015.
-
- Australian Orthopaedic Association National Joint Replacement Registry Annual Report. Adelaide, Australia: AOA; 2013. Available at: https://aoanjrr.dmac.adelaide.edu.au/annual-reports-2013. Accessed March 20, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
