

Postextubation laryngeal edema and stridor resulting in respiratory failure in critically ill adult patients: updated review
- PMID: 26395175
- PMCID: PMC4580147
- DOI: 10.1186/s13054-015-1018-2
Postextubation laryngeal edema and stridor resulting in respiratory failure in critically ill adult patients: updated review
Abstract
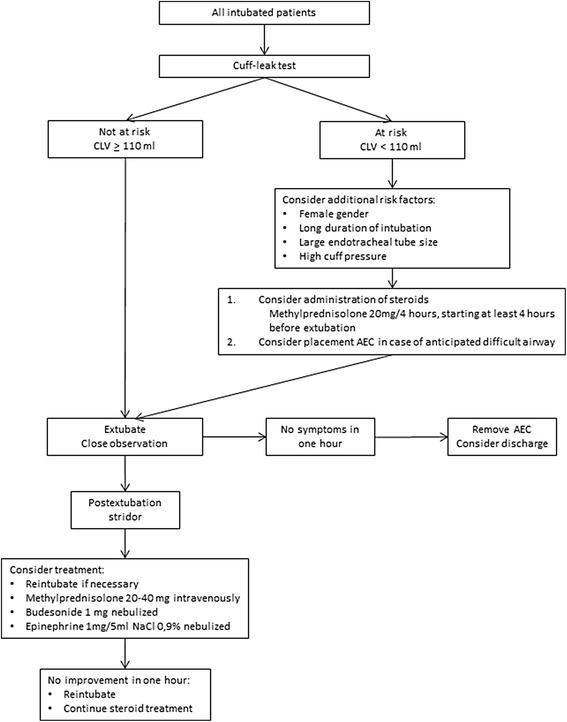
Endotracheal intubation is frequently complicated by laryngeal edema, which may present as postextubation stridor or respiratory difficulty or both. Ultimately, postextubation laryngeal edema may result in respiratory failure with subsequent reintubation. Risk factors for postextubation laryngeal edema include female gender, large tube size, and prolonged intubation. Although patients at low risk for postextubation respiratory insufficiency due to laryngeal edema can be identified by the cuff leak test or laryngeal ultrasound, no reliable test for the identification of high-risk patients is currently available. If applied in a timely manner, intravenous or nebulized corticosteroids can prevent postextubation laryngeal edema; however, the inability to identify high-risk patients prevents the targeted pretreatment of these patients. Therefore, the decision to start corticosteroids should be made on an individual basis and on the basis of the outcome of the cuff leak test and additional risk factors. The preferential treatment of postextubation laryngeal edema consists of intravenous or nebulized corticosteroids combined with nebulized epinephrine, although no data on the optimal treatment algorithm are available. In the presence of respiratory failure, reintubation should be performed without delay. Application of noninvasive ventilation or inhalation of a helium/oxygen mixture is not indicated since it does not improve outcome and increases the delay to intubation.
Figures
Comment in
-
Should Reinke edema be considered a contributing factor to post-extubation failure?Crit Care. 2015 Dec 19;19:430. doi: 10.1186/s13054-015-1147-7. Crit Care. 2015. PMID: 26683056 Free PMC article. No abstract available.
-
Value of the cuff leak test is limited.Crit Care. 2015 Dec 24;19:446. doi: 10.1186/s13054-015-1152-x. Crit Care. 2015. PMID: 26698862 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
