

Detecting Prostate Cancer
- PMID: 26396046
- PMCID: PMC4581108
- DOI: 10.3238/arztebl.2015.0605
Detecting Prostate Cancer
Abstract
Background: When prostate cancer is suspected, the prostate gland is biopsied with the aid of transrectal ultrasound (TRUS). The sensitivity of prostatic biopsy is about 50%. The fusion of magnetic resonance imaging (MRI) data with TRUS enables the targeted biopsy of suspicious areas. We studied whether this improves the detection of prostate cancer.
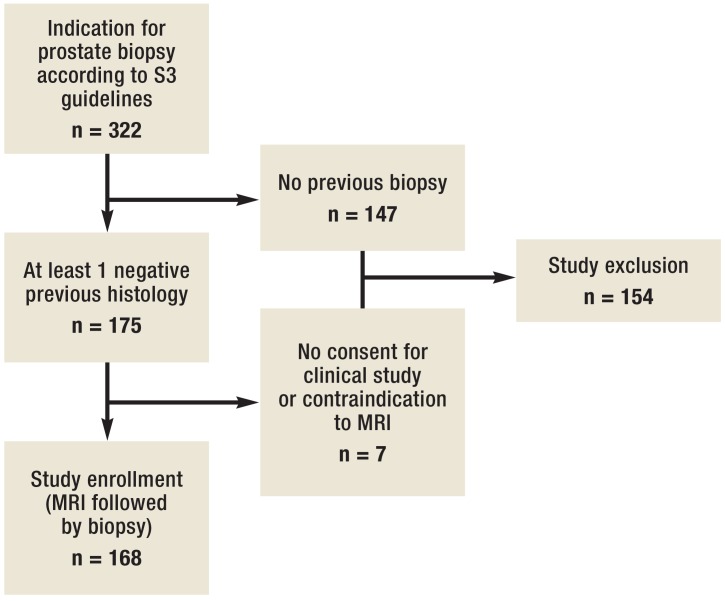
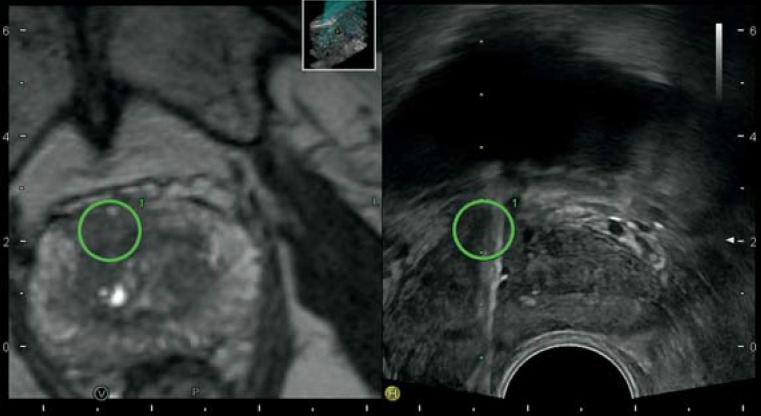
Methods: 168 men with suspected prostate cancer underwent prostate MRI after a previous negative biopsy. Suspicious lesions were assessed with the classification of the Prostate Imaging Reporting and Data System and biopsied in targeted fashion with the aid of fused MRI and TRUS. At the same sitting, a systematic biopsy with at least 12 biopsy cores was performed.
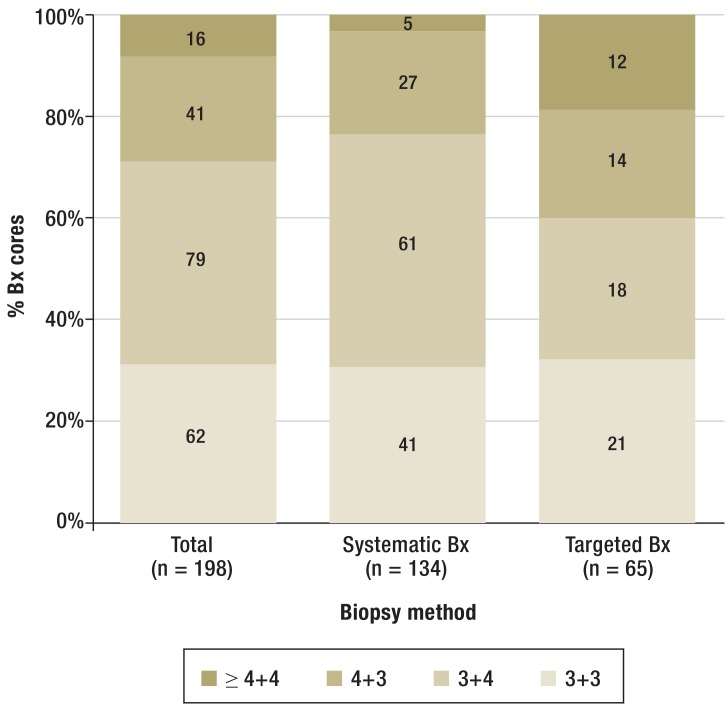
Results: Prostate cancer was detected in 71 patients (42.3%; 95% CI, 35.05-49.82). The detection rate of fusion-assisted targeted biopsy was 19% (95% CI, 13.83-25.65), compared to 37.5% (95% CI, 30.54-45.02) with systematic biopsy. Clinically significant cancer was more commonly revealed by targeted biopsy (84.4%; 95% CI, 68.25-93.14) than by systematic biopsy (65.1%; 95% CI, 52.75-75.67). In 7 patients with normal MRI findings, cancer was detected by systematic biopsy alone. Compared to systematic biopsy, targeted biopsy had a higher overall detection rate (16.5% vs. 6.3%), a higher rate of infiltration per core (30% vs. 10%), and a higher rate of detection of poorly differentiated carcinoma (18.5% vs. 3%). Patients with negative biopsies did not undergo any further observation.
Conclusion: MRI/TRUS fusion-assisted targeted biopsy improves the detection rate of prostate cancer after a previous negative biopsy. Targeted biopsy is more likely to reveal clinically significant cancer than systematic biopsy; nevertheless, systematic biopsy should still be performed, even if the MRI findings are negative.
Figures
Comment in
-
Simple Solution.Dtsch Arztebl Int. 2016 Mar 4;113(9):149. doi: 10.3238/arztebl.2016.0149a. Dtsch Arztebl Int. 2016. PMID: 26987466 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2016 Mar 4;113(9):149. doi: 10.3238/arztebl.2016.0149b. Dtsch Arztebl Int. 2016. PMID: 26987467 Free PMC article. No abstract available.
References
-
- Heidenreich A, Aus G, Bolla M, et al. EAU guidelines on prostate cancer. European urology. 2008;53:68–80. - PubMed
-
- Gosselaar C, Roobol MJ, Roemeling S, Wolters T, van Leenders GJ, Schroder FH. The value of an additional hypoechoic lesion-directed biopsy core for detecting prostate cancer. BJU international. 2008;101:685–690. - PubMed
-
- Nevoux P, Ouzzane A, Ahmed HU, et al. Quantitative tissue analyses of prostate cancer foci in an unselected cystoprostatectomy series. BJU international. 2012;110:517–523. - PubMed
-
- Haas GP, Delongchamps NB, Jones RF, et al. Needle biopsies on autopsy prostates: sensitivity of cancer detection based on true prevalence. J Natl Cancer Inst. 2007;99:1484–1489. - PubMed
-
- Walz J, Graefen M, Chun FK, et al. High incidence of prostate cancer detected by saturation biopsy after previous negative biopsy series. European urology. 2006;50:498–505. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical