

Cerebral gliosarcoma: Analysis of 16 patients and review of literature
- PMID: 26396606
- PMCID: PMC4553731
- DOI: 10.4103/1793-5482.161173
Cerebral gliosarcoma: Analysis of 16 patients and review of literature
Abstract
Background: Gliosarcoma (GS), a subtype of glioblastoma (GBM), is a rare primary neoplasm of the central nervous system. Certain features like temporal lobe affinity, tendency for extraneural metastasis and poorer outcome compared to GBM indicate that GS may indeed be a separate clinicopathologic entity. This led us to revisit this entity in our settings.
Materials and methods: Between 2009 and 2014, 16 cases of histologically proven GSs (14 primary, two secondary) were treated. Patient data were retrieved retrospectively. Statistical analysis was performed with? Statistical Package for Social Sciences, version 17.0. (Chicago, Illinois, USA). Survival was analyzed by Kaplan-Meier method.
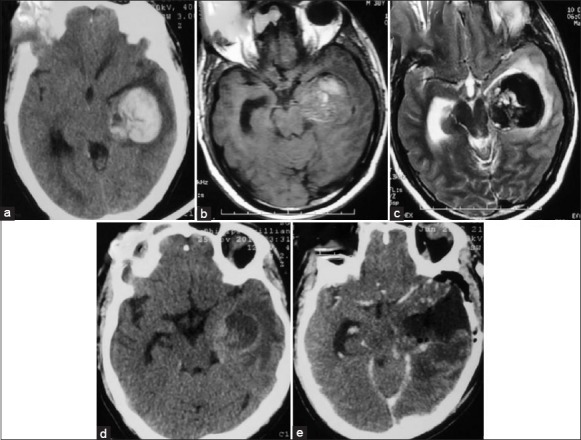
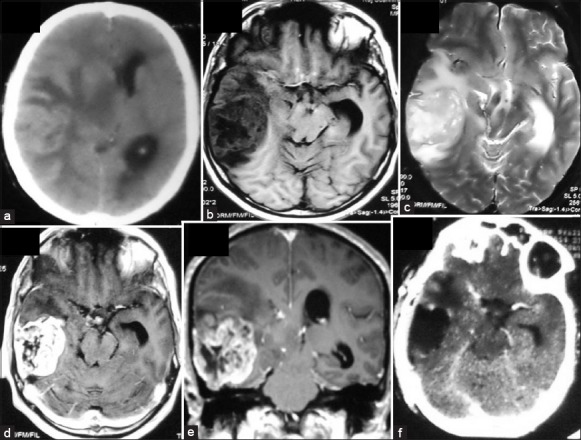
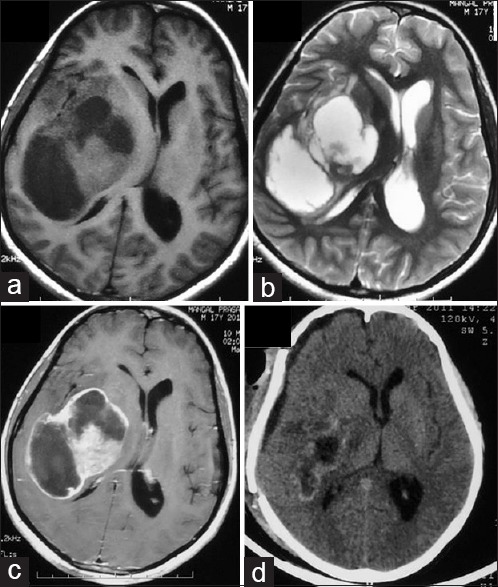
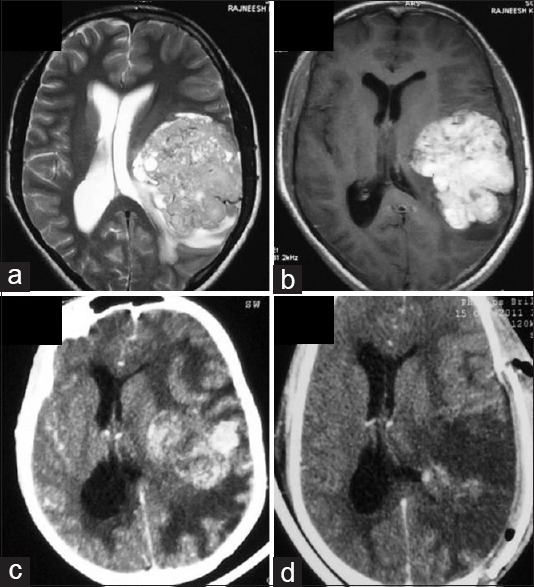
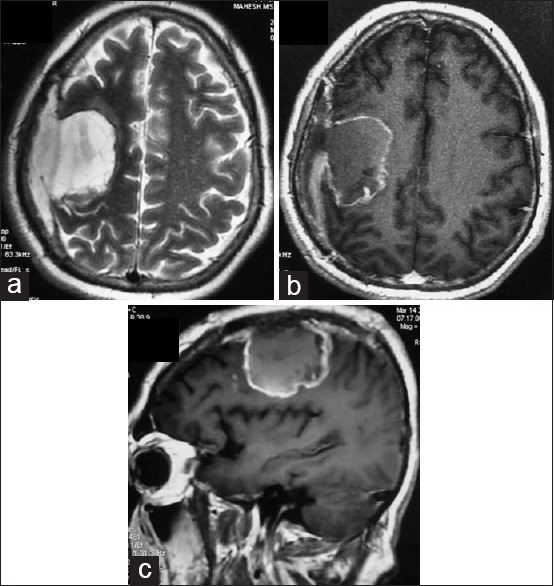
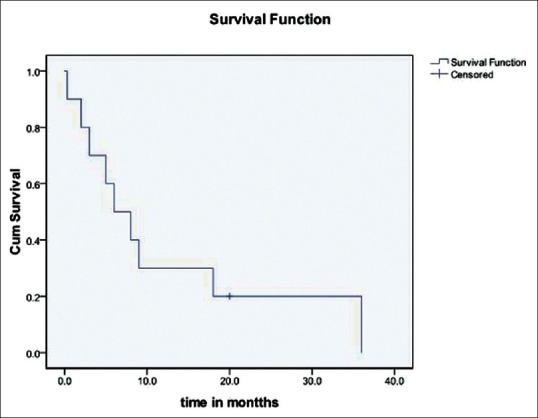
Results: GS predominantly affected males in their fifth decade of life. Raised intracranial pressure was the most common mode of clinical presentation. Temporal lobe was the most commonly affected part of the brain and majority of primary and all of secondary GBM were located peripherally. In 7 (43.8%) patients, tumor was radiologically well-demarcated and enhanced strongly and homogenously on contrast as compared to 9 (56.2%) patients where the tumor was ill-defined and showed heterogenous patchy or ring enhancement. Extent of excision was total in seven patients (43.8%), near total in 4 (25%) and subtotal in five patients (31.2%). Median survival was 6 months. Patients with well-demarcated, enhancing mass on imaging intraoperatively had firm tumors with a good plane of cleavage and had a better survival (8 months) compared to those in whom the tumor radiologically and intraoperatively mimicked GBM (2 months).
Conclusion: GS is associated with poor survival (median survival 6 months). Radiological and intraoperative findings help categorize these tumors into GBM like GS and meningioma like GS. While the former histologically mimics GBM and has very poor survival (2 months), GS with meningioma like feature tends to have better survival (8 months).
Keywords: Chemotherapy; glioblastoma; gliosarcoma; immunohistochemistry; pathology; surgery; survival.
Figures
References
-
- Stroebe H. Uber Entstehung und Bau der Gehirngliome. Beitr Pathol Anat Allg Pathol. 1895;18:405–86.
-
- Morantz RA, Feigen I, Ransohoff J. Clinical and pathological study of 24 cases of gliosarcoma. J Neurosurg. 1976;45:398–408. - PubMed
-
- Meis JM, Martz Kl, Nelson JS. Mixed glioblastoma multiforme and sarcoma. A clinicopathologic study of 26 Radiation Therapy Oncology Group cases. Cancer. 1991;67:2342–9. - PubMed
-
- Perry JR, Ang LC, Bilbao JM, Muller PJ. Clinicopathologic features of prima- ry and postradiation cerebral gliosarcoma. Cancer. 1995;75:2910–18. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous