

Changing Trends in Adenoidectomy
- PMID: 26396947
- PMCID: PMC4571468
- DOI: 10.1007/s12070-013-0698-7
Changing Trends in Adenoidectomy
Abstract
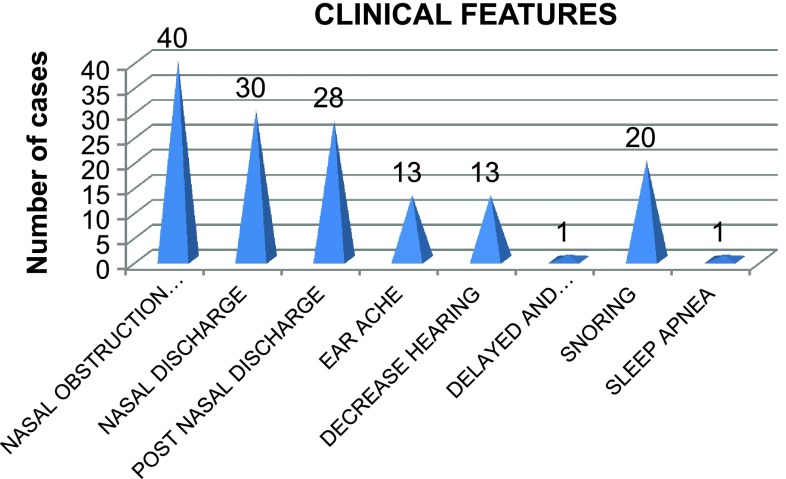
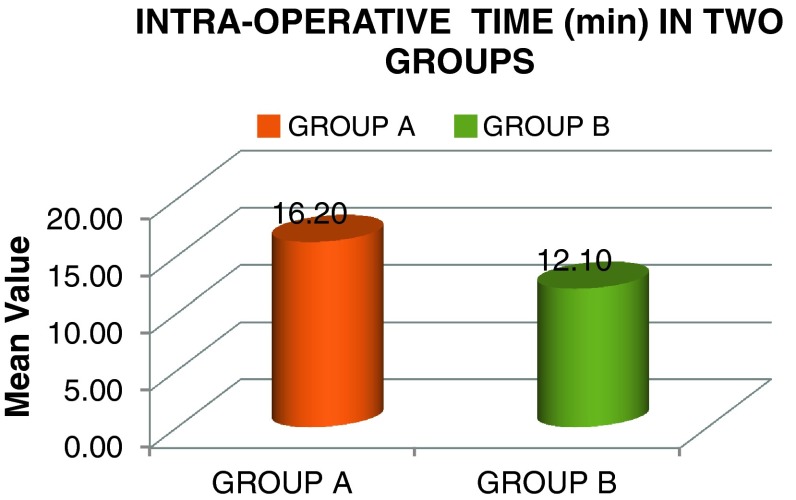
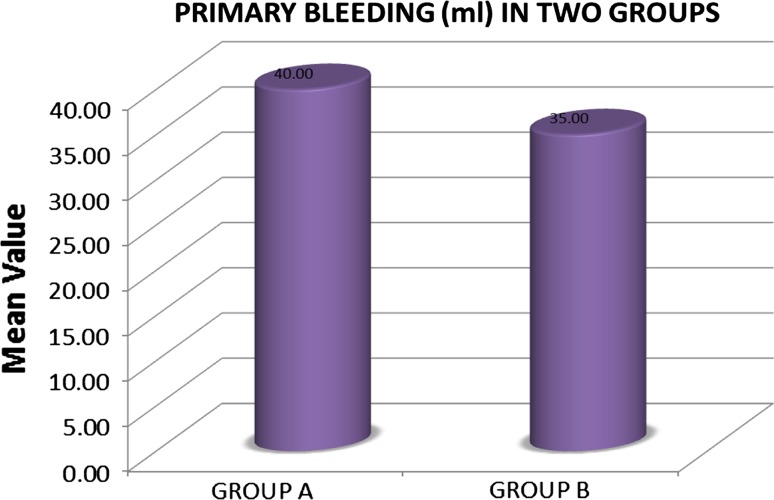
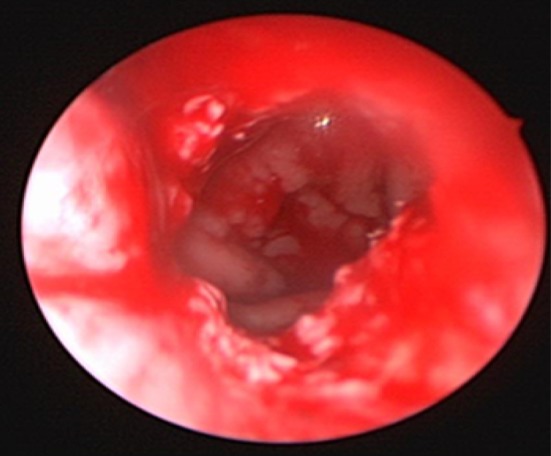
Adenoid hypertrophy treatment is must to alleviate chronic nasal obstruction, mouth breathing, rhinosinusitis and eustachian tube dysfunction. For proper management of this clinical entity a thorough clinical examination along with radiological and endoscopic evaluation is mandatory. Although, few children having adenoid hypertrophy respond to medical treatment, surgery remains the mainstay. An adenoidectomy can be performed by variety of techniques. Conventional adenoidectomy is by the curettage method, still practiced in many institutions, though, a recent technique of endoscopic assisted adenoidectomy by microdebrider is also getting popularized. Both the techniques have their own merits and demerits. However, which of the two surgical techniques is better, is still a matter of preference and experience of the surgeon with the technique. In the present study we will compare the conventional curettage adenoidectomy with endoscopically assisted adenoidectomy done with microdebrider in 40 pediatric patients of adenoid hypertrophy.
Keywords: Adenoidectomy; Compare; Endoscopically; Microdebrider.
Figures


Similar articles
-
Adenoidectomy in Children: What Is the Evidence and What Is its Role?Curr Otorhinolaryngol Rep. 2018;6(1):64-73. doi: 10.1007/s40136-018-0190-8. Epub 2018 Mar 2. Curr Otorhinolaryngol Rep. 2018. PMID: 32226659 Free PMC article. Review.
-
Comparison between curettage adenoidectomy and endoscopic-assisted microdebrider adenoidectomy in terms of Eustachian tube dysfunction.Braz J Otorhinolaryngol. 2020 Jan-Feb;86(1):38-43. doi: 10.1016/j.bjorl.2018.08.004. Epub 2018 Sep 25. Braz J Otorhinolaryngol. 2020. PMID: 30322828 Free PMC article. Clinical Trial.
-
Combined Conventional and Endoscopic Microdebrider-Assisted Adenoidectomy: A Tertiary Centre Experience.J Clin Diagn Res. 2017 Feb;11(2):MC05-MC07. doi: 10.7860/JCDR/2017/24682.9394. Epub 2017 Feb 1. J Clin Diagn Res. 2017. PMID: 28384895 Free PMC article.
-
Comparative outcomes of microdebrider adenoidectomy, curettage adenoidectomy through oral cavity under 70 endoscope, and endoscopic transoral low-temperature ablation for adenoid hypertrophy.Int J Pediatr Otorhinolaryngol. 2024 Nov;186:112143. doi: 10.1016/j.ijporl.2024.112143. Epub 2024 Oct 20. Int J Pediatr Otorhinolaryngol. 2024. PMID: 39476644
-
Coblator adenoidectomy in pediatric patients: a state-of-the-art review.Eur Arch Otorhinolaryngol. 2023 Oct;280(10):4339-4349. doi: 10.1007/s00405-023-08094-7. Epub 2023 Jul 26. Eur Arch Otorhinolaryngol. 2023. PMID: 37493842 Free PMC article. Review.
Cited by
-
Comparison of transnasal and transoral routes of microdebrider combined curettage adenoidectomy and assessment of endoscopy for residue: a randomized prospective study.Eur Arch Otorhinolaryngol. 2021 Mar;278(3):797-805. doi: 10.1007/s00405-020-06385-x. Epub 2020 Sep 28. Eur Arch Otorhinolaryngol. 2021. PMID: 32989492 Clinical Trial.
-
[The etiology and related factors of Eustachian tube dysfunction].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021 Dec;35(12):1137-1140. doi: 10.13201/j.issn.2096-7993.2021.12.018. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021. PMID: 34886633 Free PMC article. Review. Chinese.
-
Adenoidectomy in Children: What Is the Evidence and What Is its Role?Curr Otorhinolaryngol Rep. 2018;6(1):64-73. doi: 10.1007/s40136-018-0190-8. Epub 2018 Mar 2. Curr Otorhinolaryngol Rep. 2018. PMID: 32226659 Free PMC article. Review.
-
Endoscopic Adenoidectomy Replacing the Outdated Curette Adenoidectomy: Comparison of the Two Methods at a Tertiary Care Centre.Indian J Otolaryngol Head Neck Surg. 2022 Dec;74(Suppl 3):4788-4794. doi: 10.1007/s12070-022-03089-y. Epub 2022 Mar 21. Indian J Otolaryngol Head Neck Surg. 2022. PMID: 36742736 Free PMC article.
-
Comparison of Conventional Curettage Adenoidectomy Versus Endoscopic Powered Adenoidectomy: A Randomised Single-Blind Study.Indian J Otolaryngol Head Neck Surg. 2022 Oct;74(Suppl 2):1044-1049. doi: 10.1007/s12070-020-02122-2. Epub 2020 Sep 2. Indian J Otolaryngol Head Neck Surg. 2022. PMID: 36452556 Free PMC article.
References
-
- Hall MJ, Lawrence L. Ambulatory surgery in the United States, 1996. Adv Data Vital Health Stat. 1998;300:1–16. - PubMed
-
- Hall MJ, Lawrence L. Ambulatory surgery in the United States, 1996. Adv Data Vital Health Stat. 2006;33(6):573–581. - PubMed
-
- Benito Orejas JI, Alonso Mesonero M, Almaraz Gomez A, Morais Perez D, Santos Perez J. Trend changes in the adenotonsillar surgery. Otorhinolaryngol Ibero Am. 2006;33(6):573–581. - PubMed
-
- Becker DG. Powered instrumentation in surgery of the nose and paranasal sinuses. Otolaryngol Head Neck Surg. 2000;8(1):18–21.
LinkOut - more resources
Full Text Sources
Other Literature Sources