

Nandrolone Plus Moderate Exercise Increases the Susceptibility to Lethal Arrhythmias
- PMID: 26396972
- PMCID: PMC4576214
- DOI: 10.5812/cardiovascmed.26233v2
Nandrolone Plus Moderate Exercise Increases the Susceptibility to Lethal Arrhythmias
Abstract
Background: Until now, no experimental study has directly assessed the arrhythmogenesis of chronic consumption of anabolic androgenic steroids along with moderate-intensity endurance exercise.
Objectives: We evaluated the influence of integration of anabolic androgenic steroids along with moderate-intensity endurance exercise on susceptibility to lethal ventricular arrhythmias in rat.
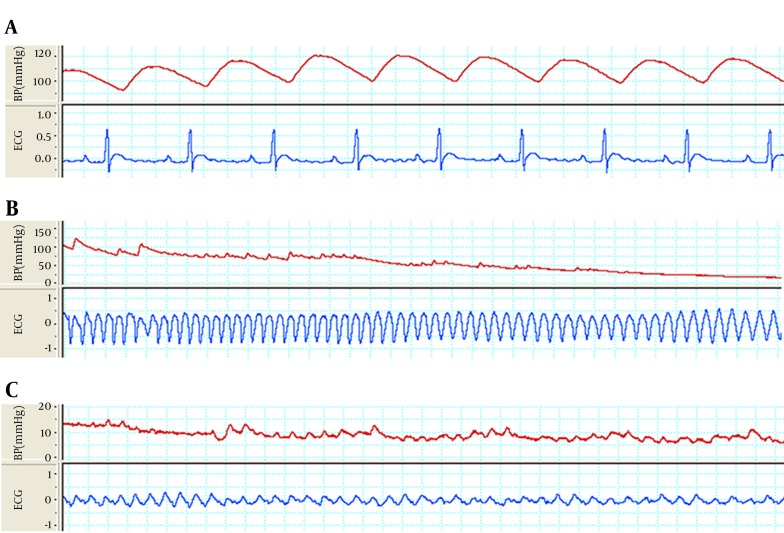
Materials and methods: The animal groups were as follows: control group (CTL); exercise group (EX) which were under 6 weeks of treadmill exercise; nandrolone group (Nan) which received 5 mg/kg of nandrolone decanoate twice a week; vehicle group (Arach) which received Arachis oil (solvent of nandrolone); trained vehicle group (Arach + Ex); and trained nandrolone group (Nan + Ex). One day after ending of the intervention period, arrhythmia was inducted by intravenous infusion of aconitine and ventricular arrhythmias were recorded. Then malondialdehyde (MDA) and glutathione peroxidase (GPX) of heart tissue were measured.
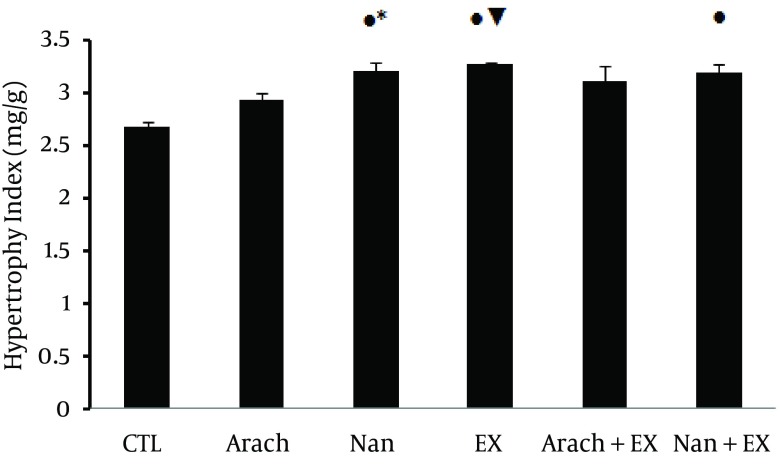
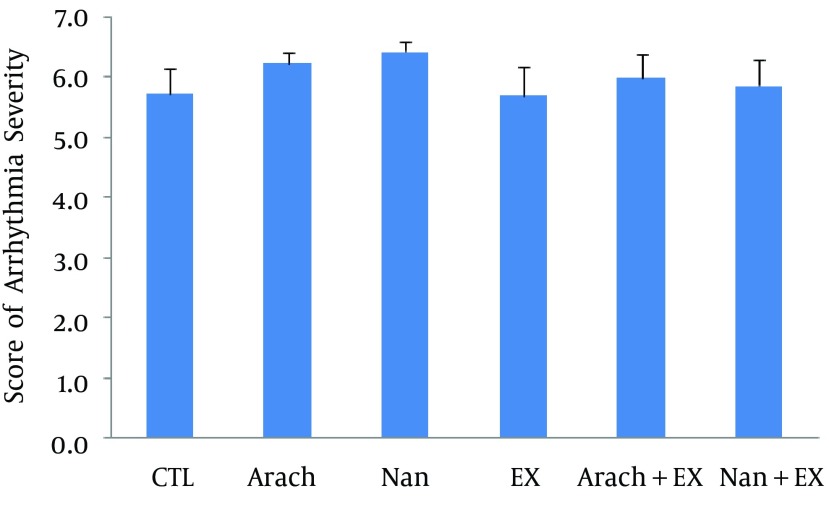
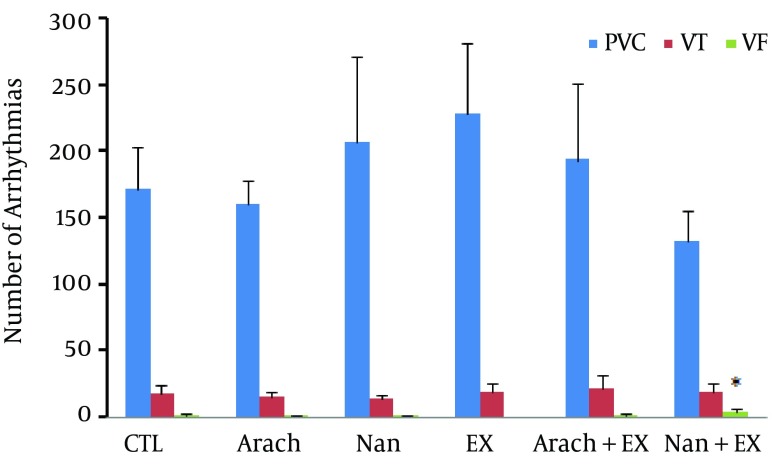
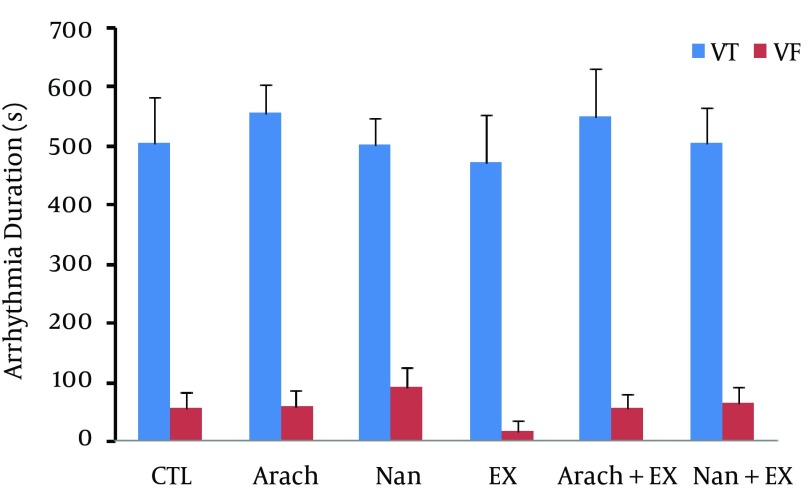
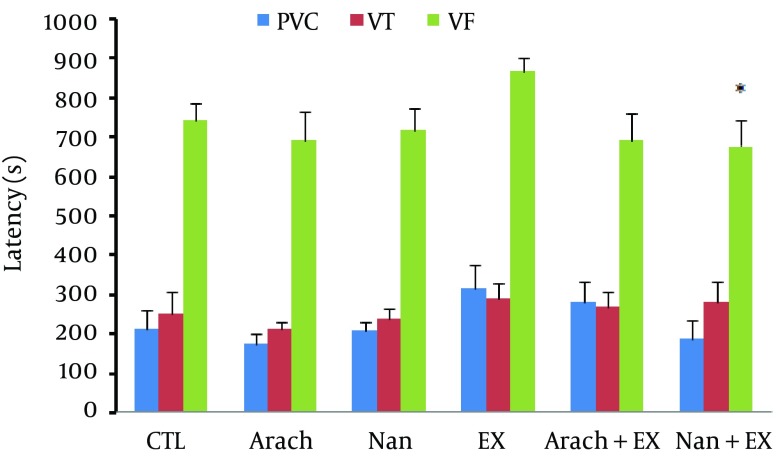
Results: Nandrolone, exercise, and their combination were associated with heart hypertrophy. Exercise could prevent the incremental effect of nandrolone on MDA/GPX ratio. Chronic administration of nandrolone with moderate-intensity endurance exercise had no significant effect on blood pressure, heart rate, and basal electrocardiographic parameters. Combination of nandrolone and exercise significantly increased the incidence of ventricular fibrillation (VF) and reduced the VF latency (P < 0.05).
Conclusions: The findings suggest that chronic coadministration of nandrolone with moderate-intensity endurance exercise facilitates the VF occurrence in rat. Complementary studies are needed to elucidate the involved mechanisms of this abnormality.
Keywords: Aerobic Exercise; Nandrolone Decanoate; Ventricular Fibrillation.
Figures
References
-
- Sullivan ML, Martinez CM, Gennis P, Gallagher EJ. The cardiac toxicity of anabolic steroids. Prog Cardiovasc Dis. 1998;41(1):1–15. - PubMed
-
- Golestani R, Slart RH, Dullaart RP, Glaudemans AW, Zeebregts CJ, Boersma HH, et al. Adverse cardiovascular effects of anabolic steroids: pathophysiology imaging. Eur J Clin Invest. 2012;42(7):795–803. - PubMed
-
- Demirel HA, Powers SK, Zergeroglu MA, Shanely RA, Hamilton K, Coombes J, et al. Short-term exercise improves myocardial tolerance to in vivo ischemia-reperfusion in the rat. J Appl Physiol (1985). 2001;91(5):2205–12. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources