

Variation in the Contents of Sepsis Bundles and Quality Measures. A Systematic Review
- PMID: 26397842
- PMCID: PMC4724896
- DOI: 10.1513/AnnalsATS.201503-163BC
Variation in the Contents of Sepsis Bundles and Quality Measures. A Systematic Review
Abstract
Rationale: Sepsis contributes to one in every two to three inpatient hospital deaths. Early recognition and treatment are instrumental in reducing mortality, yet there are substantial quality gaps. Sepsis bundles containing quality metrics are often used in efforts to improve outcomes. Several prominent organizations have published their own bundles, but there are few head-to-head comparisons of content.
Objectives: We sought to determine the degree of agreement on component elements of sepsis bundles and the associated timing goals for completion of each element. We additionally sought to evaluate the amount of variation between metrics associated with bundles.
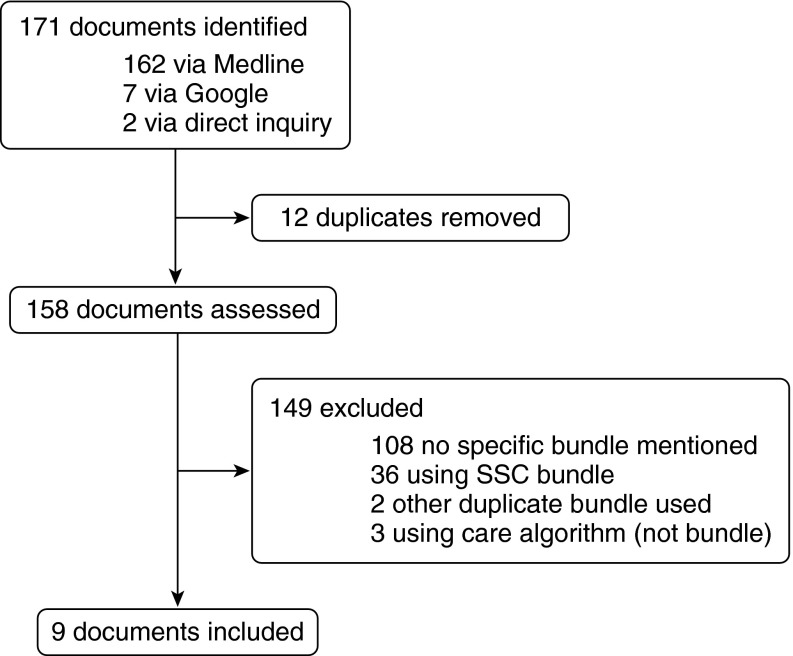
Methods: We reviewed the components of and level of agreement among several sepsis resuscitation and management bundles. We compared the individual bundle elements, together with their associated goals and metrics. We performed a systematic review (PubMed 2008-2015) and searched publically available online content, supplemented by interviews with key informants, to identify eight distinct bundles. Bundles are presented as current as of April 2015.
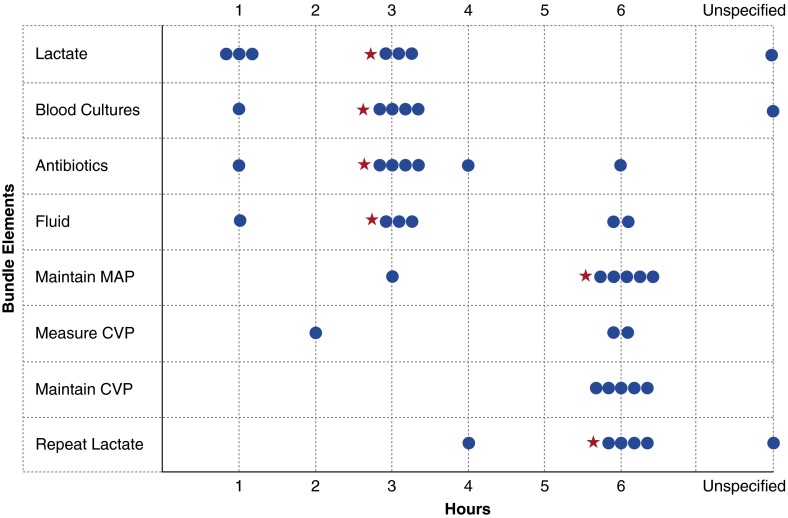
Measurements and main results: Broadly, elements of care covered early resuscitation and short-term management. Bundles varied from 6 to 10 elements, and there were 12 distinct elements listed across all bundles. Only lactate collection and broad-spectrum antibiotics were common to all eight bundles, although there were seven elements included in at least 75% of the bundles. Timing goals for the collection of lactate and antibiotic administration varied among bundles from within 1 to 6 hours of diagnosis or admission. Notably, no bundle included metrics evaluating timeliness or completeness of sepsis recognition.
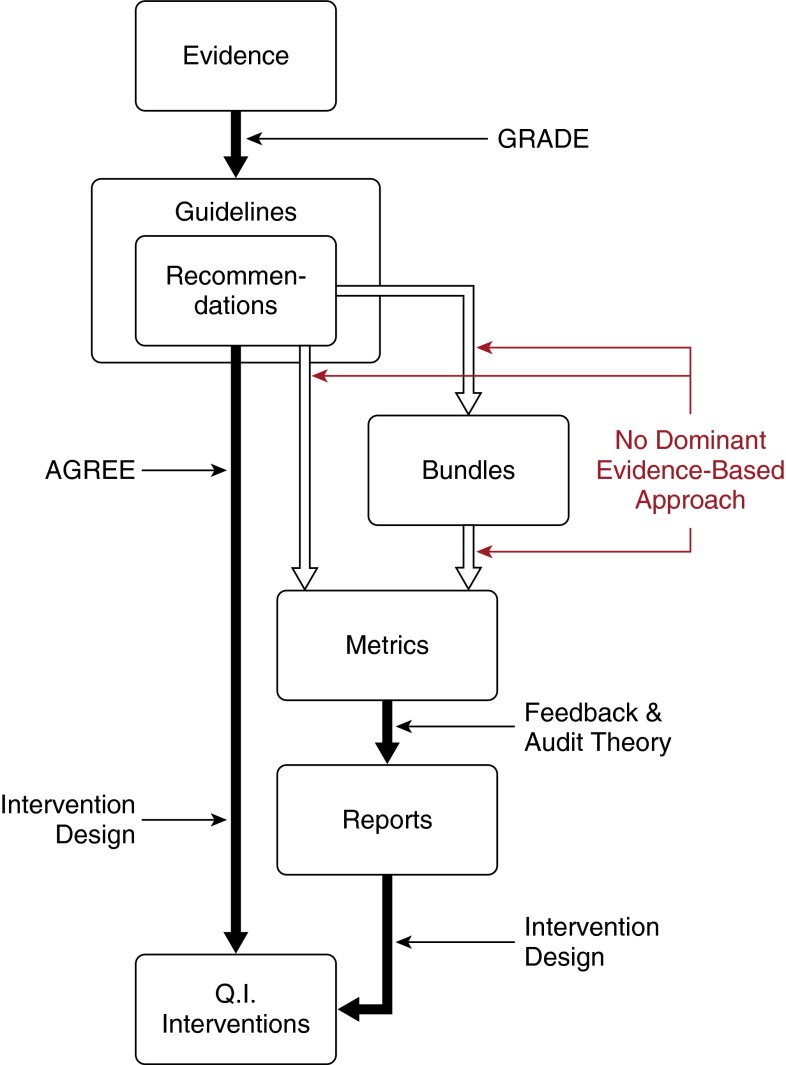
Conclusions: There is a lack of consensus on component elements and timing goals across highly recognized sepsis bundles. These differences highlight an urgent need for comparative effectiveness research to guide future implementation and for metrics to evaluate progress. None of the widely instituted bundles include metrics to evaluate sepsis recognition or diagnostic accuracy.
Keywords: bundles; guidelines; quality improvement; quality metrics; sepsis.
Figures
Comment in
-
Variation and Cost-effectiveness of Quality Measurement Programs. The Case of Sepsis Bundles.Ann Am Thorac Soc. 2015 Nov;12(11):1597-9. doi: 10.1513/AnnalsATS.201509-625ED. Ann Am Thorac Soc. 2015. PMID: 26540416 No abstract available.
References
-
- Liu V, Escobar GJ, Greene JD, Soule J, Whippy A, Angus DC, Iwashyna TJ. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312:90–92. - PubMed
-
- Lagu T, Rothberg MB, Shieh MS, Pekow PS, Steingrub JS, Lindenauer PK. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40:754–761. - PubMed
-
- Torio CM, Andrews RM. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet] Rockville (MD): Agency for Health Care Policy and Research (US); 2006–2013; National inpatient hospital costs: the most expensive conditions by payer, 2011: statistical brief #160. - PubMed
-
- Centers for Medicare and Medicaid ServicesNew Medicare data available to increase transparency on hospital utilization [Internet]. [accessed 2015 June 29]. Available from: http://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-s...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
