

The Effects of Alternative Resuscitation Strategies on Acute Kidney Injury in Patients with Septic Shock
- PMID: 26398704
- PMCID: PMC4803059
- DOI: 10.1164/rccm.201505-0995OC
The Effects of Alternative Resuscitation Strategies on Acute Kidney Injury in Patients with Septic Shock
Abstract
Rationale: Septic shock is a common cause of acute kidney injury (AKI), and fluid resuscitation is a major part of therapy.
Objectives: To determine if structured resuscitation designed to alter fluid, blood, and vasopressor use affects the development or severity of AKI or outcomes.
Methods: Ancillary study to the ProCESS (Protocolized Care for Early Septic Shock) trial of alternative resuscitation strategies (two protocols vs. usual care) for septic shock.
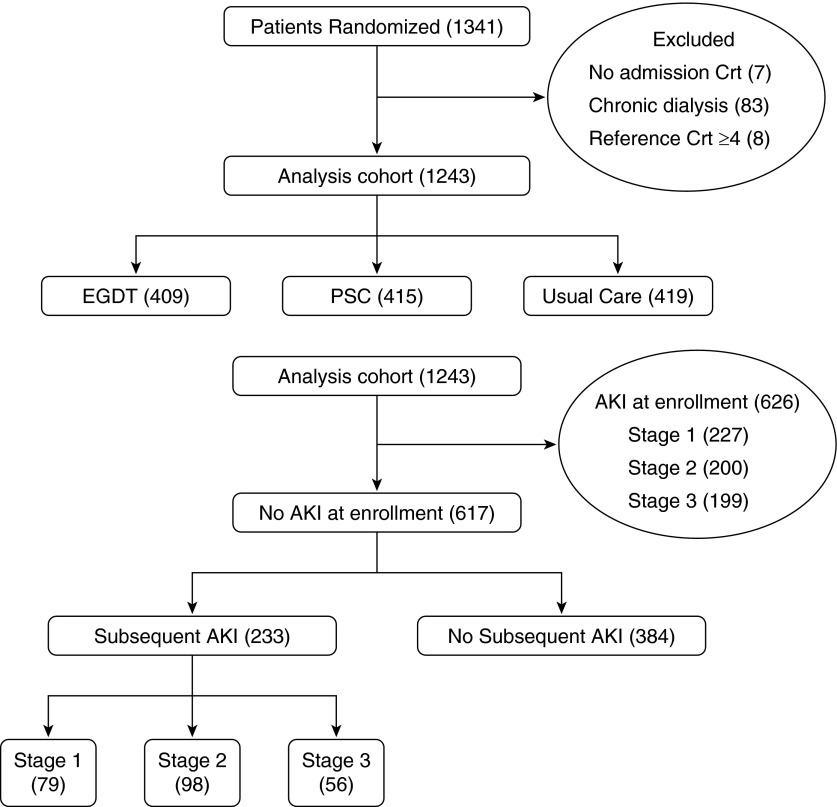
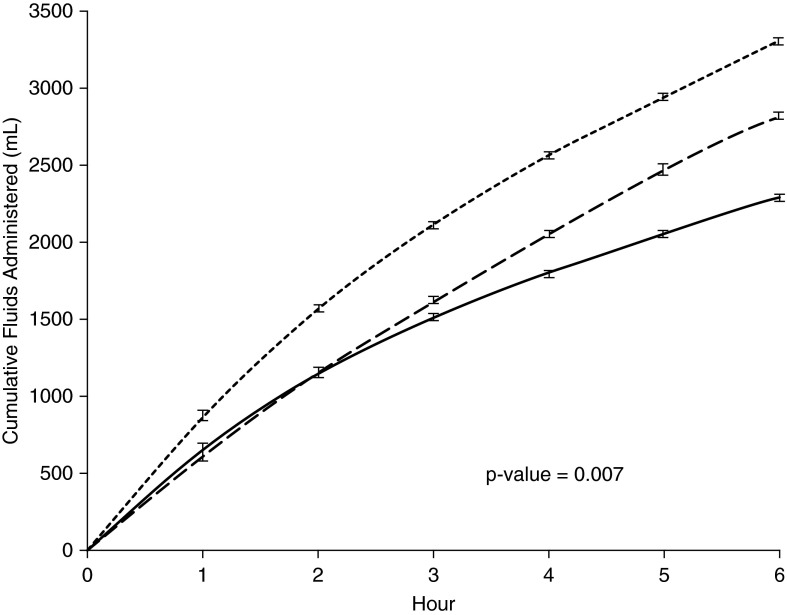
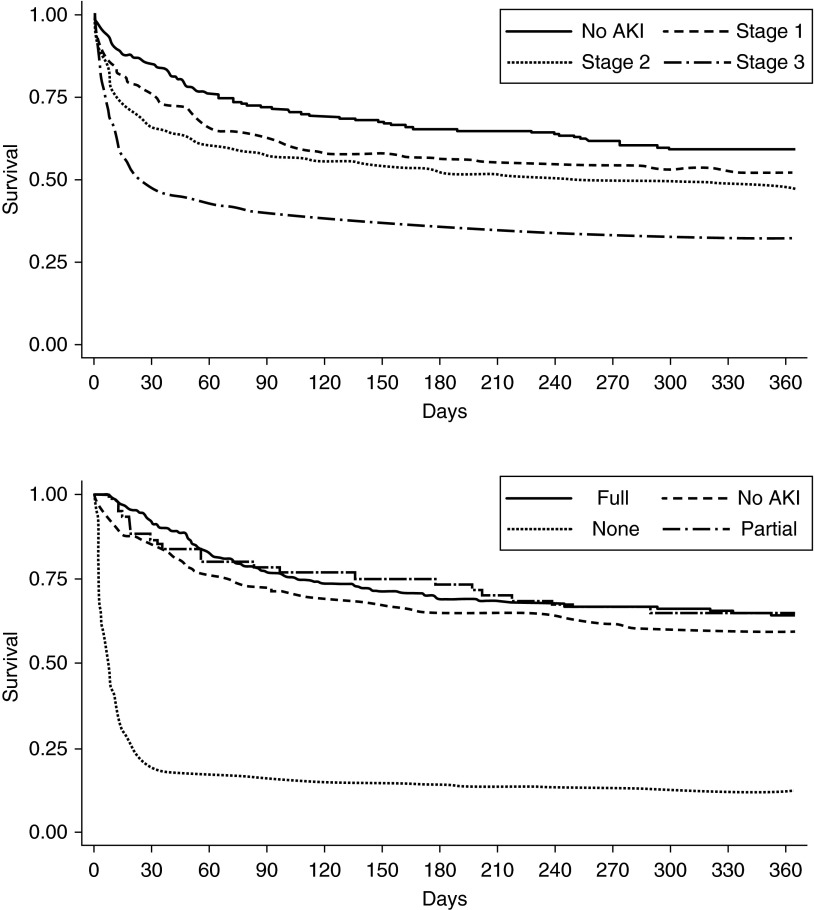
Measurements and main results: We studied 1,243 patients and classified AKI using serum creatinine and urine output. We determined recovery status at hospital discharge, examined rates of renal replacement therapy and fluid overload, and measured biomarkers of kidney damage. Among patients without evidence of AKI at enrollment, 37.6% of protocolized care and 38.1% of usual care patients developed kidney injury (P = 0.90). AKI duration (P = 0.59) and rates of renal replacement therapy did not differ between study arms (6.9% for protocolized care and 4.3% for usual care; P = 0.08). Fluid overload occurred in 8.3% of protocolized care and 6.3% of usual care patients (P = 0.26). Among patients with severe AKI, complete and partial recovery was 50.7 and 13.2% for protocolized patients and 49.1 and 13.4% for usual care patients (P = 0.93). Sixty-day hospital mortality was 6.2% for patients without AKI, 16.8% for those with stage 1, and 27.7% for stages 2 to 3.
Conclusions: In patients with septic shock, AKI is common and associated with adverse outcomes, but it is not influenced by protocolized resuscitation compared with usual care.
Keywords: acute kidney injury; early goal-directed therapy; resuscitation; sepsis; septic shock.
Figures
Comment in
-
Treating Acute Kidney Injury. One Less Weapon in the Armamentarium?Am J Respir Crit Care Med. 2016 Feb 1;193(3):232-3. doi: 10.1164/rccm.201509-1900ED. Am J Respir Crit Care Med. 2016. PMID: 26829419 No abstract available.
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, et al. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. - PubMed
-
- Sutherland SM, Zappitelli M, Alexander SR, Chua AN, Brophy PD, Bunchman TE, Hackbarth R, Somers MJG, Baum M, Symons JM, et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: the prospective pediatric continuous renal replacement therapy registry. Am J Kidney Dis. 2010;55:316–325. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
