

Metabolomic profiles of hepatocellular carcinoma in a European prospective cohort
- PMID: 26399231
- PMCID: PMC4581424
- DOI: 10.1186/s12916-015-0462-9
Metabolomic profiles of hepatocellular carcinoma in a European prospective cohort
Abstract
Background: Hepatocellular carcinoma (HCC), the most prevalent form of liver cancer, is difficult to diagnose and has limited treatment options with a low survival rate. Aside from a few key risk factors, such as hepatitis, high alcohol consumption, smoking, obesity, and diabetes, there is incomplete etiologic understanding of the disease and little progress in identification of early risk biomarkers.
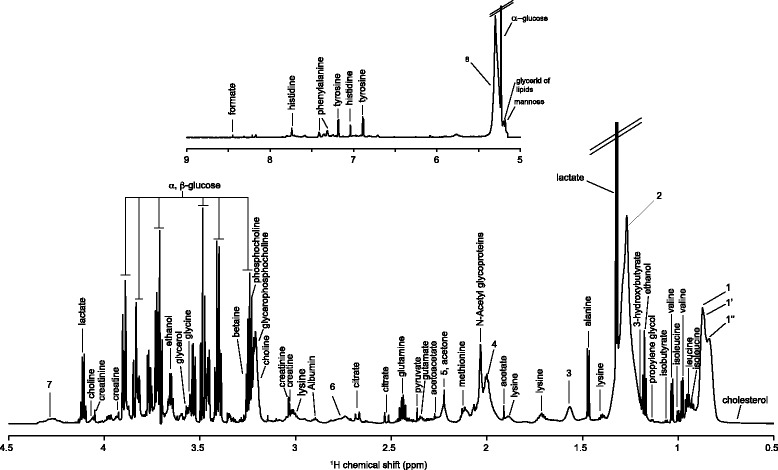
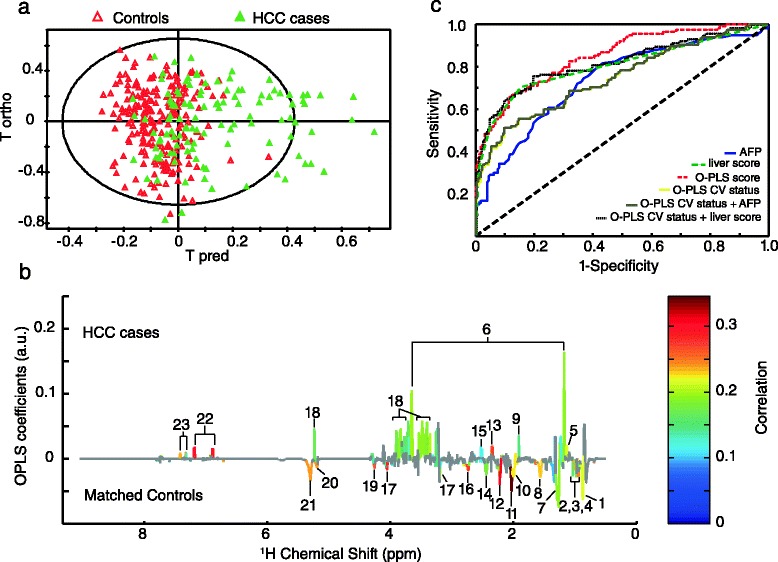
Methods: To address these aspects, an untargeted nuclear magnetic resonance metabolomic approach was applied to pre-diagnostic serum samples obtained from first incident, primary HCC cases (n = 114) and matched controls (n = 222) identified from amongst the participants of a large European prospective cohort.
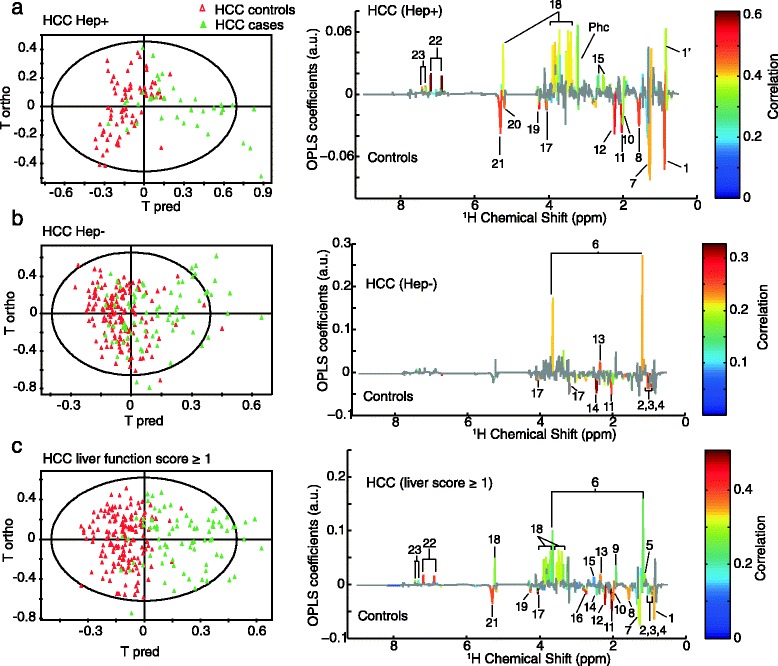
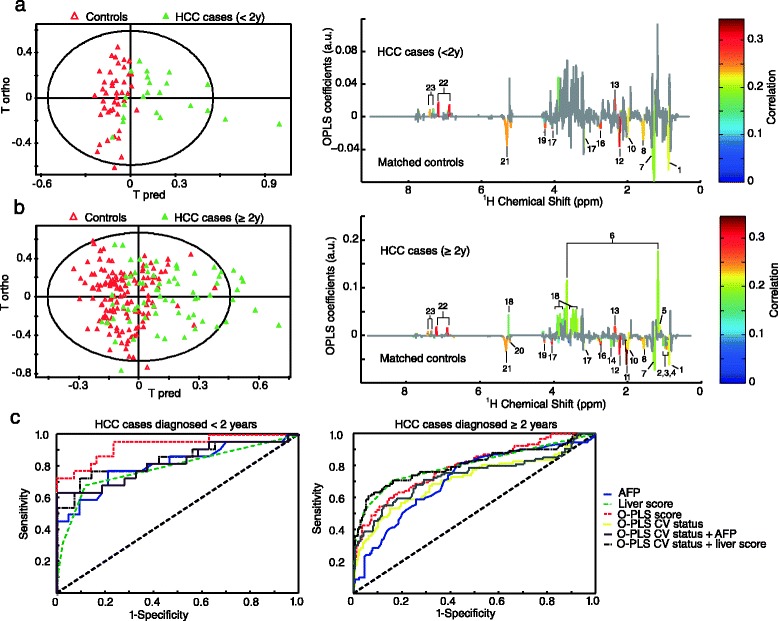
Results: A metabolic pattern associated with HCC risk comprised of perturbations in fatty acid oxidation and amino acid, lipid, and carbohydrate metabolism was observed. Sixteen metabolites of either endogenous or exogenous origin were found to be significantly associated with HCC risk. The influence of hepatitis infection and potential liver damage was assessed, and further analyses were made to distinguish patterns of early or later diagnosis.
Conclusion: Our results show clear metabolic alterations from early stages of HCC development with application for better etiologic understanding, prevention, and early detection of this increasingly common cancer.
Figures
References
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide 2013. http://globocan.iarc.fr, accessed on 30/01/2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
