

Relationship between fibroblastic foci profusion and high resolution CT morphology in fibrotic lung disease
- PMID: 26399508
- PMCID: PMC4581474
- DOI: 10.1186/s12916-015-0479-0
Relationship between fibroblastic foci profusion and high resolution CT morphology in fibrotic lung disease
Abstract
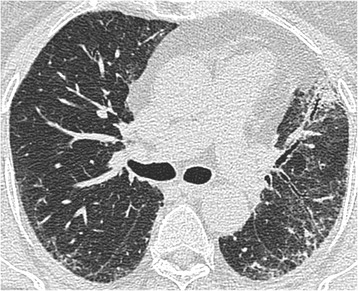
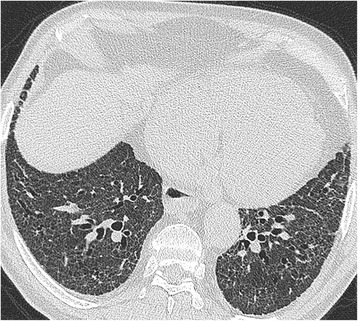
Background: Fibroblastic foci profusion on histopathology and severity of traction bronchiectasis on highresolution computed tomography (HRCT) have been shown to be predictors of mortality in patients with idiopathic pulmonary fibrosis (IPF). The aim of this study was to investigate the relationship between fibroblastic foci (FF) profusion and HRCT patterns in patients with a histopathologic diagnosis of usual interstitial pneumonia (UIP), fibrotic non-specific interstitial pneumonia (NSIP) and chronic hypersensitivity pneumonitis (CHP).
Methods: The HRCT scans of 162 patients with a histopathologic diagnosis of UIP or fibrotic NSIP (n = 162) were scored on extent of groundglass opacification, reticulation, honeycombing, emphysema and severity of traction bronchiectasis. For each patient, a fibroblastic foci profusion score based on histopathologic appearances was assigned. Relationships between extent of fibroblastic foci and individual HRCT patterns were investigated using univariate correlation analysis and multivariate linear regression.
Results: Increasing extent of reticulation (P < 0.0001) and increasing severity of traction bronchiectasis (P < 0.0001) were independently associated with increasing FF score within the entire cohort. Within individual multidisciplinary team diagnosis subgroups, the only significant independent association with FF score was severity of traction bronchiectasis in patients with idiopathic pulmonary fibrosis (IPF)/UIP (n = 66, r(2) = 0.19, P < 0.0001) and patients with chronic hypersensitivity pneumonitis (CHP) (n = 49, r(2) = 0.45, P < 0.0001). Furthermore, FF score had the strongest association with severity of traction bronchiectasis in patients with IPF (r(2) = 0.34, P < 0.0001) and CHP (r(2) = 0.35, P < 0.0001). There was no correlation between FF score and severity of traction bronchiectasis in patients with fibrotic NSIP. Global disease extent had the strongest association with severity of traction bronchiectasis in patients with fibrotic NSIP (r(2) = 0.58, P < 0.0001).
Conclusion: In patients with fibrotic lung disease, profusion of fibroblastic foci is strikingly related to the severity of traction bronchiectasis, particularly in IPF and CHP. This may explain the growing evidence that traction bronchiectasis is a predictor of mortality in several fibrotic lung diseases.
Figures

References
-
- Walsh SL, Sverzellati N, Devaraj A, Keir GJ, Wells AU, Hansell DM. Connective tissue disease related fibrotic lung disease: high resolution computed tomographic and pulmonary function indices as prognostic determinants. Thorax. 2013. - PubMed
-
- Walsh SL, Sverzellati N, Devaraj A, Wells AU, Hansell DM. Chronic hypersensitivity pneumonitis: high resolution computed tomography patterns and pulmonary function indices as prognostic determinants. Eur Radiol. 2012. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
