

Respiratory and limb muscle dysfunction in pulmonary arterial hypertension: a role for exercise training?
- PMID: 26401245
- PMCID: PMC4556495
- DOI: 10.1086/682431
Respiratory and limb muscle dysfunction in pulmonary arterial hypertension: a role for exercise training?
Abstract
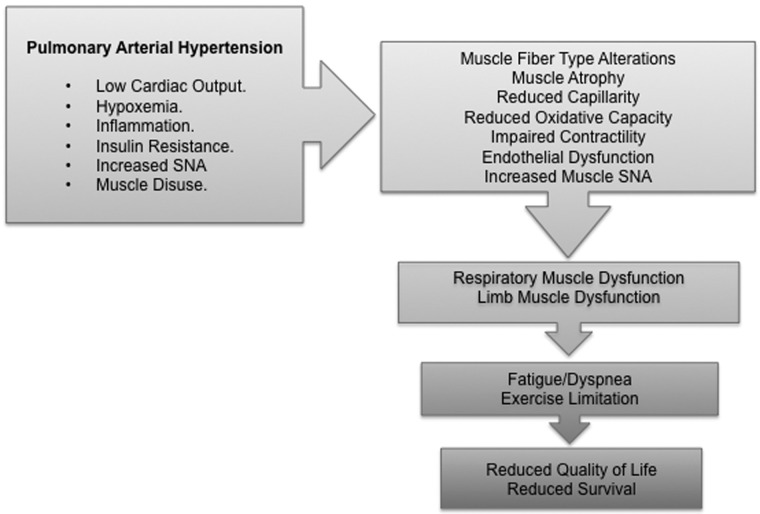
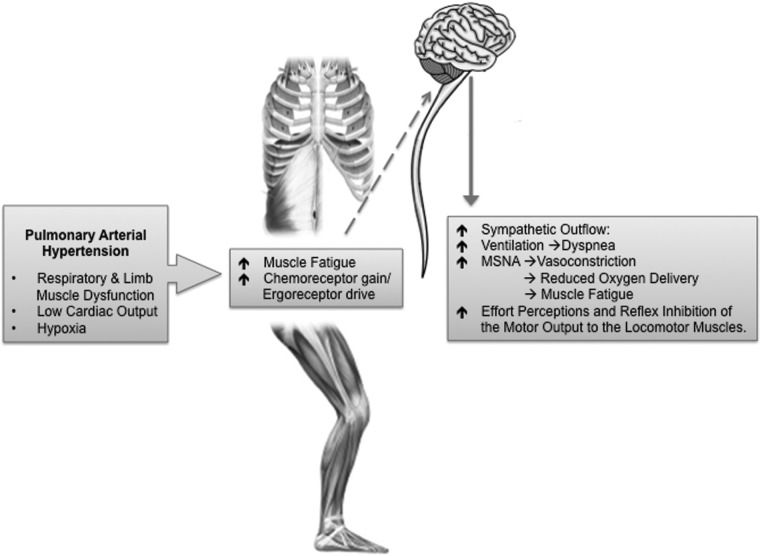
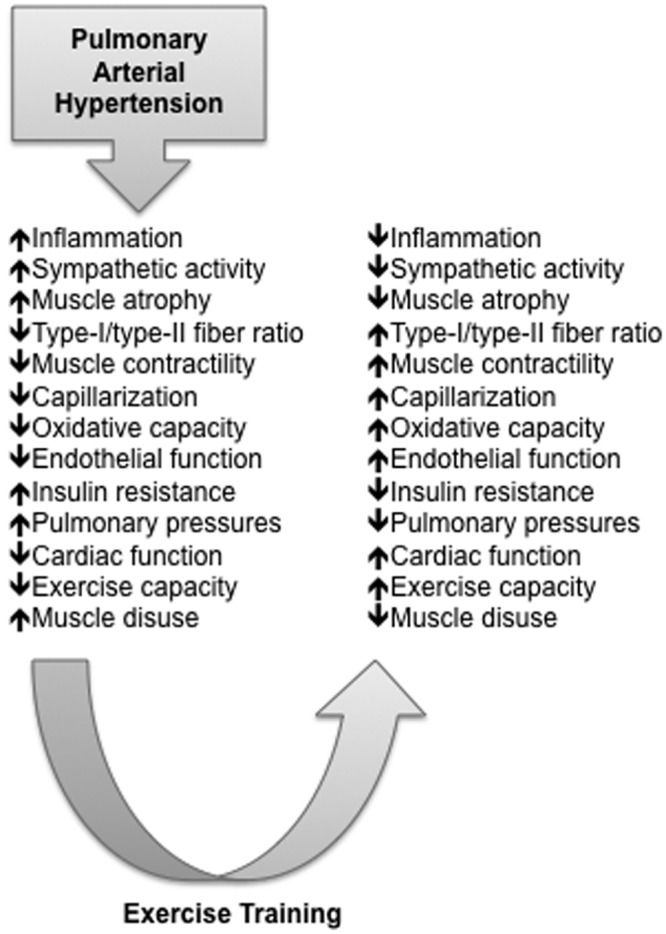
Respiratory and limb muscle dysfunction is emerging as an important pathophysiological abnormality in pulmonary arterial hypertension (PAH). Muscle abnormalities appear to occur frequently and promote dyspnea, fatigue, and exercise limitation in patients with PAH. Preliminary data suggest that targeted muscle training may be of benefit, although further evidence is required to consolidate these findings into specific recommendations for exercise training in patients with PAH. This article reviews the current evidence on prevalence, risk factors, and implications of respiratory and limb muscle dysfunction in patients with PAH. It also reviews the impact of exercise rehabilitation on morphologic, metabolic, and functional muscle profile and outcomes in PAH. Future research priorities are highlighted.
Keywords: pulmonary arterial hypertension; rehabilitation; respiratory muscles; skeletal muscle.
Figures
References
-
- Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiéry JL, Barberà JA, Beghetti M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009;30(20):2493–2537. - PubMed
-
- Naeije R. Breathing more with weaker respiratory muscles in pulmonary arterial hypertension. Eur Respir J 2005;25(1):6–8. - PubMed
-
- Garcia-Aymerich J, Serra I, Gómez FP, Farrero E, Balcells E, Rodriguez DA, de Batlle J, et al. Physical activity and clinical and functional status in COPD. Chest 2009;136(1):62–70. - PubMed
-
- Agustí A. Systemic effects of chronic obstructive pulmonary disease: what we know and what we don’t know (but should). Proc Am Thorac Soc 2007;4(7):522–525. - PubMed
-
- Yndestad A, Damås JK, Øie E, Ueland T, Gullestad L, Aukrust P. Systemic inflammation in heart failure—the whys and wherefores. Heart Fail Rev 2006;11(1):83–92. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
