

Intravenous iron therapy in patients with idiopathic pulmonary arterial hypertension and iron deficiency
- PMID: 26401247
- PMCID: PMC4556497
- DOI: 10.1086/682217
Intravenous iron therapy in patients with idiopathic pulmonary arterial hypertension and iron deficiency
Abstract
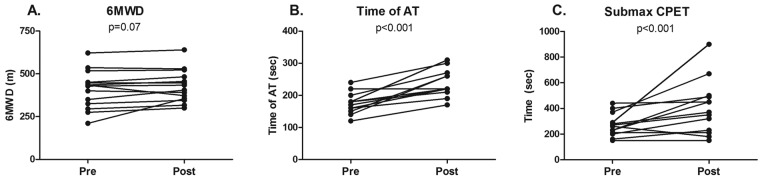
In patients with idiopathic pulmonary arterial hypertension (iPAH), iron deficiency is common and has been associated with reduced exercise capacity and worse survival. Previous studies have shown beneficial effects of intravenous iron administration. In this study, we investigated the use of intravenous iron therapy in iron-deficient iPAH patients in terms of safety and effects on exercise capacity, and we studied whether altered exercise capacity resulted from changes in right ventricular (RV) function and skeletal muscle oxygen handling. Fifteen patients with iPAH and iron deficiency were included. Patients underwent a 6-minute walk test, cardiopulmonary exercise tests, cardiac magnetic resonance imaging, and a quadriceps muscle biopsy and completed a quality-of-life questionnaire before and 12 weeks after receiving a high dose of intravenous iron. The primary end point, 6-minute walk distance, was not significantly changed after 12 weeks (409 ± 110 m before vs. 428 ± 94 m after; P = 0.07). Secondary end points showed that intravenous iron administration was well tolerated and increased body iron stores in all patients. In addition, exercise endurance time (P < 0.001) and aerobic capacity (P < 0.001) increased significantly after iron therapy. This coincided with improved oxygen handling in quadriceps muscle cells, although cardiac function at rest and maximal [Formula: see text] were unchanged. Furthermore, iron treatment was associated with improved quality of life (P < 0.05). In conclusion, intravenous iron therapy in iron-deficient iPAH patients improves exercise endurance capacity. This could not be explained by improved RV function; however, increased quadriceps muscle oxygen handling may play a role. (
Trial registration: ClinicalTrials.gov identifier NCT01288651).
Keywords: exercise capacity; iron; right ventricle; skeletal muscle.
Figures
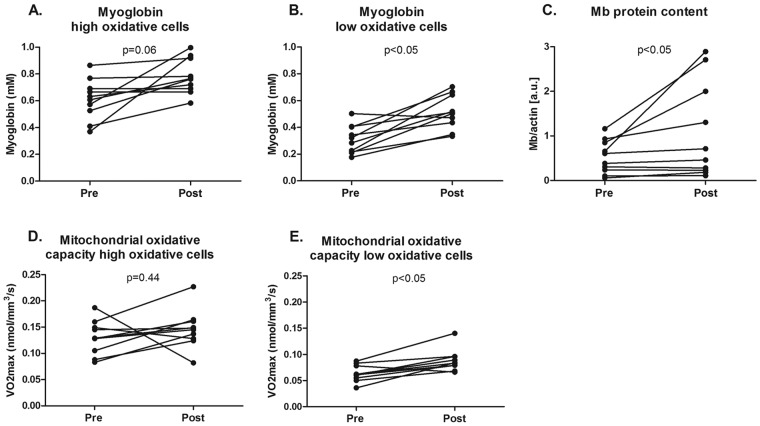
 ) in high oxidative cells, was unchanged by iron therapy (D). In low oxidative cells,
) in high oxidative cells, was unchanged by iron therapy (D). In low oxidative cells,  was higher after iron therapy (E).
was higher after iron therapy (E).
References
References Cited Only in the Appendix
-
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002;166:111–117. - PubMed
-
- ERS Task Force on Standardization of Clinical Exercise Testing. Clinical exercise testing with reference to lung diseases: indications, standardization and interpretation strategies. Eur Respir J 1997;10:2662–2689. - PubMed
-
- Quanjer PH, Tammeling GJ, Cotes JE, et al. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl 1993;16:5–40. - PubMed
-
- Cotes JE, Chinn DJ, Quanjer PH, et al. Standardization of the measurement of transfer factor (diffusing capacity). Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl 1993;16:41–52. - PubMed
-
- van de Veerdonk MC, Kind T, Marcus JT, et al. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J Am Coll Cardiol 2011;58:2511–2519. - PubMed
References
-
- Rhodes CJ, Howard LS, Busbridge M, et al. Iron deficiency and raised hepcidin in idiopathic pulmonary arterial hypertension: clinical prevalence, outcomes, and mechanistic insights. J Am Coll Cardiol 2011;58:300–309. - PubMed
-
- Ruiter G, Lankhorst S, Boonstra A, et al. Iron deficiency is common in idiopathic pulmonary arterial hypertension. Eur Respir J 2011;37:1386–1391. - PubMed
-
- Soon E, Treacy CM, Toshner MR, et al. Unexplained iron deficiency in idiopathic and heritable pulmonary arterial hypertension. Thorax 2011;66:326–332. - PubMed
-
- Brownlie T, Utermohlen V, Hinton PS, et al. Tissue iron deficiency without anemia impairs adaptation in endurance capacity after aerobic training in previously untrained women. Am J Clin Nutr 2004;79:437–443. - PubMed
-
- Anker SD, Comin CJ, Filippatos G, et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med 2009;361:2436–2448. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
