

Neurocognitive decline in HIV patients is associated with ongoing T-cell activation in the cerebrospinal fluid
- PMID: 26401512
- PMCID: PMC4574808
- DOI: 10.1002/acn3.227
Neurocognitive decline in HIV patients is associated with ongoing T-cell activation in the cerebrospinal fluid
Abstract
Objective: HIV-associated neurocognitive disorders (HAND) remain a challenge despite combination antiretroviral therapy (cART). Immune cell activation has been implicated to play a major role in the development of HAND.
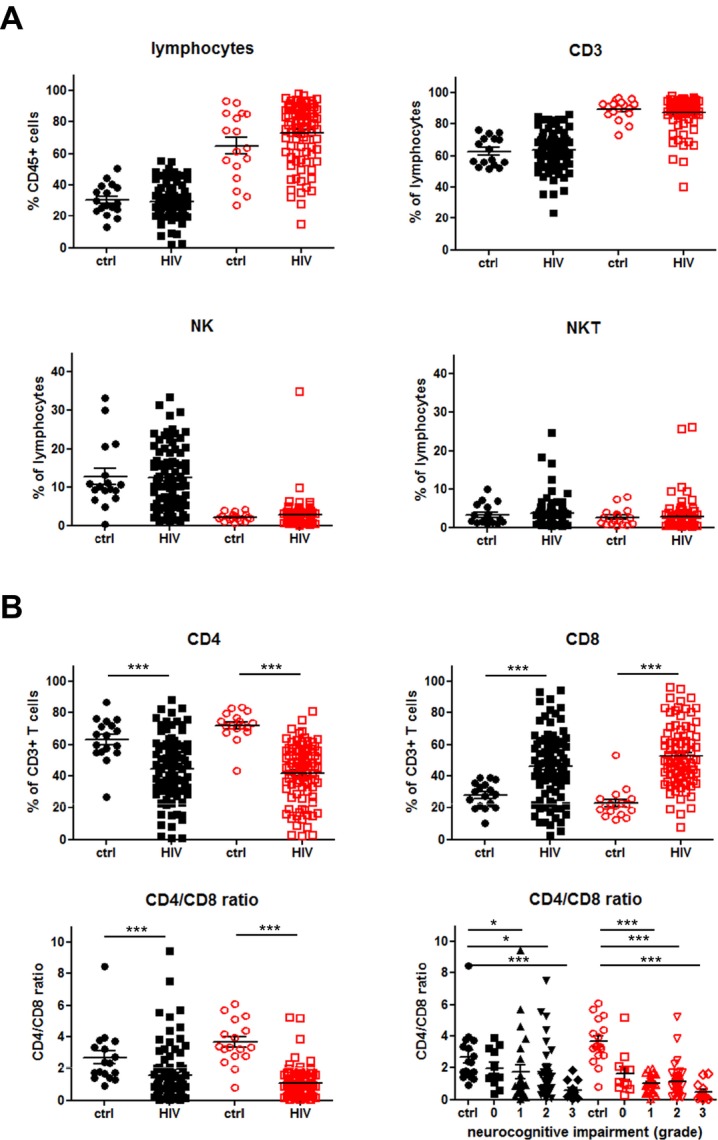
Methods: In this study, we used multicolor flow cytometry on peripheral blood (PB) and cerebrospinal fluid (CSF) samples to determine the expression of HLA-DR and programmed death-1 (PD-1) on CD4+ and CD8+ T cells in patients with chronic HIV infection. Expression levels were correlated with HI virus load in PB and CSF, classification of HAND and severity of magnetic resonance imaging (MRI) signal abnormalities.
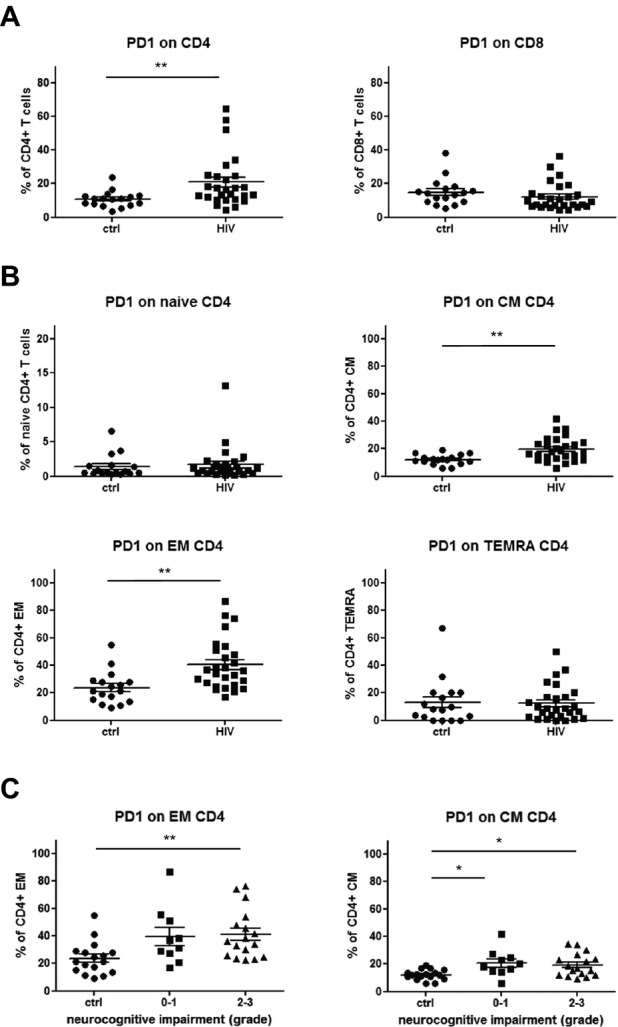
Results: In a cohort of 86 HIV patients we found that the grade of neurocognitive impairment and the severity of MRI signal abnormalities correlated with decreasing CD4/CD8-ratios and increased frequencies of HLA-DR expressing CD4+ and CD8+ T cells reaching the highest values in the CSF samples. Importantly, HLA-DR upregulation was still detectable in virologically suppressed HIV patients. Further, T-cell subpopulation analysis of 40 HIV patients showed a significant shift from naïve to effector memory (EM) T cells that was negatively correlated with the grade of neurocognitive impairment in the PB samples. Moreover, PD-1 was significantly increased on CD4+ memory T cells with highest levels on EM T cells in HIV patients with mild or severe neurocognitive alterations.
Interpretation: The CD4/CD8 ratio, the proportion of EM to naïve T cells and the immune activation profile of CD4+ and CD8+ T cells in PB and CSF might be useful parameters to monitor the efficacy of cART and to identify HIV patients at risk of further neurocognitive deterioration.
Figures



References
-
- Antinori A, Ammassari A, De Luca A, et al. Diagnosis of AIDS-related focal brain lesions: a decision-making analysis based on clinical and neuroradiologic characteristics combined with polymerase chain reaction assays in CSF. Neurology. 1997;48:687–694. - PubMed
-
- McArthur JC, Hoover DR, Bacellar H, et al. Dementia in AIDS patients: incidence and risk factors. Multicenter AIDS Cohort Study. Neurology. 1993;43:2245–2252. - PubMed
-
- McArthur JC, Selnes OA, Glass JD, et al. HIV dementia. Incidence and risk factors. Res Publ Assoc Res Nerv Ment Dis. 1994;72:251–272. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
