

Dose and timing in neurorehabilitation: prescribing motor therapy after stroke
- PMID: 26402404
- PMCID: PMC4643742
- DOI: 10.1097/WCO.0000000000000256
Dose and timing in neurorehabilitation: prescribing motor therapy after stroke
Abstract
Purpose of review: Prescribing the most appropriate dose of motor therapy for individual patients is a challenge because minimal data are available and a large number of factors are unknown. This review explores the concept of dose and reviews the most recent findings in the field of neurorehabilitation, with a focus on relearning motor skills after stroke.
Recent findings: Appropriate dosing involves the prescription of a specific amount of an active ingredient, at a specific frequency and duration. Dosing parameters, particularly amount, are not well defined or quantified in most studies. Compiling data across studies indicates a positive, moderate dose-response relationship, indicating that more movement practice results in better outcomes. This relationship is confounded by time after stroke, however, wherein longer durations of scheduled therapy may not be beneficial in the first few hours, days, and/or weeks.
Summary: These findings suggest that substantially more movement practice may be necessary to achieve better outcomes for people living with the disabling consequences of stroke. Preclinical investigations are needed to elucidate many of the unknowns and allow for a more biologically driven rehabilitation prescription process. Likewise, clinical investigations are needed to determine the dose-response relationships and examine the potential dose-timing interaction in humans.
Conflict of interest statement
Conflicts of interest: none
Figures
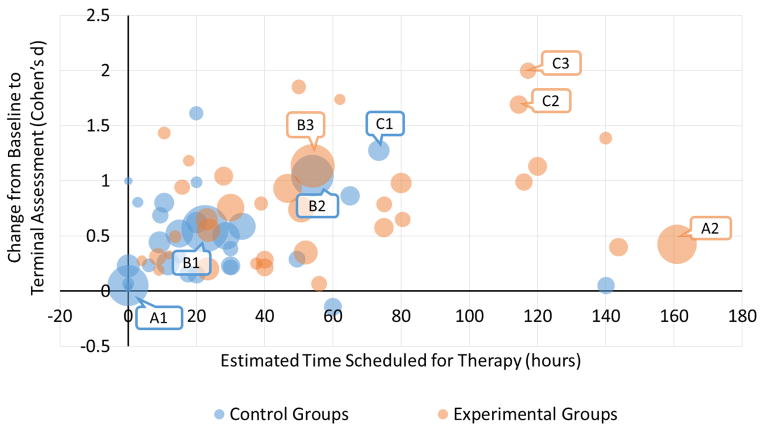
A1: Standard care, prior to crossover
A2: Constraint induced movement therapy
B1: Standard care, prior to crossover
B2: Home physical therapy, focused on functional strengthening and balance
B3: Early locomotor training, body-weight supported treadmill training + over-ground training
C1: Standard/conventional therapy
C2: Intensive arm-focused training
C3: Intensive leg-focused training
References
-
- Kwakkel G, Wagenaar RC, Twisk JW, Lankhorst GJ, Koetsier JC. Intensity of leg and arm training after primary middle-cerebral-artery stroke. A randomised trial. Lancet. 1999;354(9174):191–196. - PubMed
-
- Kwakkel G, Kollen B, Lindeman E. Understanding the pattern of functional recovery after stroke: Facts and theories. Restor Neurol Neurosci. 2004;22(3–5):281–299. - PubMed
-
- Galvin R, Murphy B, Cusack T, Stokes E. The impact of increased duration of exercise therapy on functional recovery following stroke--what is the evidence? Top Stroke Rehabil. 2008;15(4):365–377. - PubMed
-
- Veerbeek JM, Koolstra M, Ket JC, van Wegen EE, Kwakkel G. Effects of augmented exercise therapy on outcome of gait and gait-related activities in the first 6 months after stroke: A meta-analysis. Stroke. 2011;42(11):3311–3315. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
